Download to read offline
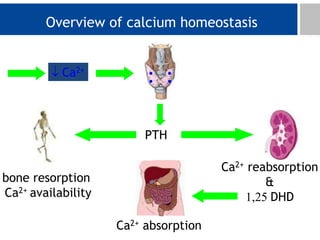
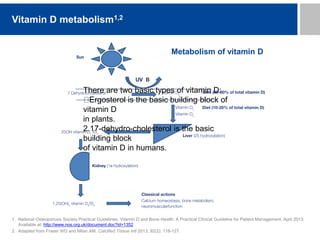
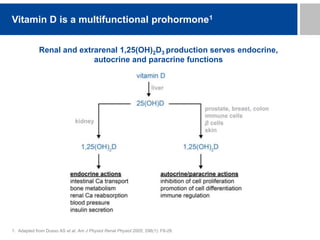
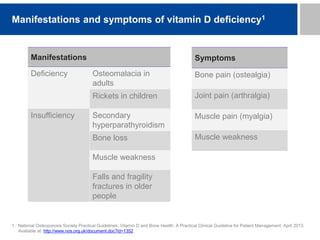
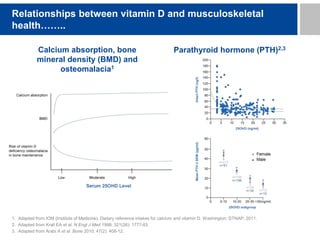
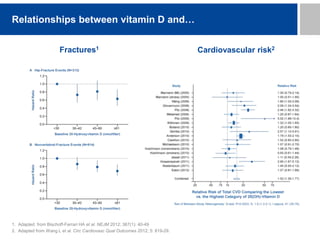
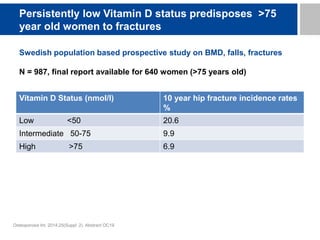
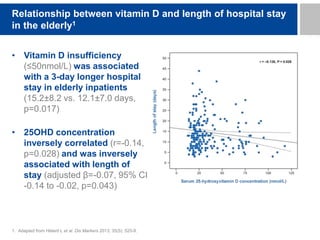
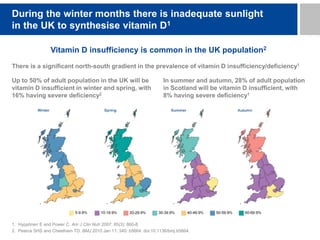
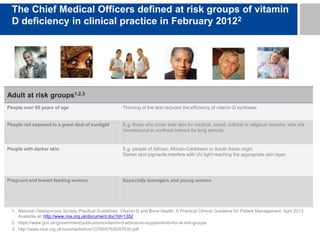
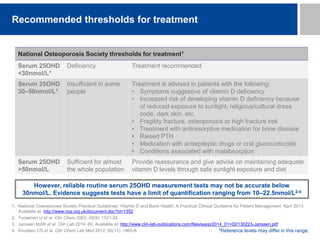
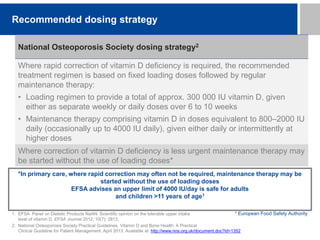
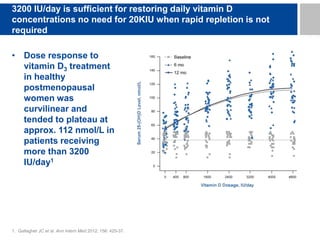

This document summarizes guidelines for managing vitamin D deficiency and osteoporosis. It discusses vitamin D metabolism and functions, manifestations of deficiency, relationships between vitamin D and bone and cardiovascular health, risk groups for deficiency in the UK, recommended thresholds and dosing strategies for treatment, and recommendations regarding supplements for pregnant/breastfeeding women. It also notes that high calcium doses are not needed to treat vitamin D deficiency alone, and that licensed preparations should be used where possible.





























































