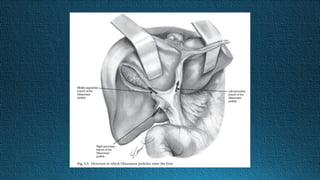
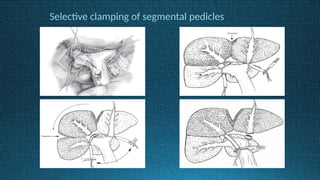
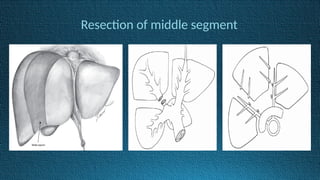
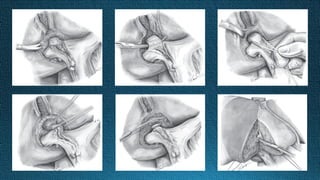
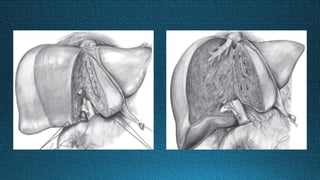
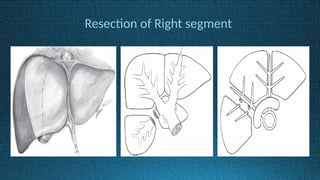
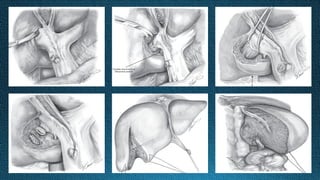
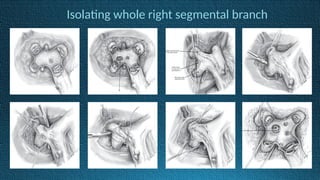
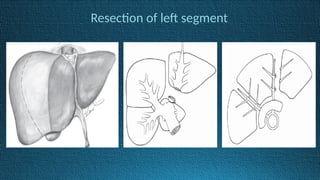
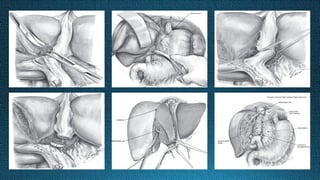
The document discusses the evolution and techniques of liver resection, highlighting the glissonian pedicle approach developed over several decades. This method is described as safe and feasible, offering advantages such as shorter operation times, less blood loss, and reduced surgeon stress. Key challenges include handling pedicles carefully and addressing tumors near the hepatic hilum.