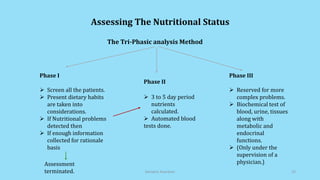
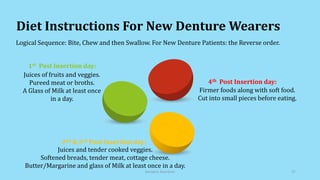
The document discusses geriatric nutrition, emphasizing the importance of proper dietary practices to address the unique nutritional needs of the elderly. It covers factors affecting nutritional status, nutrient requirements for aging individuals, and recommendations for specific dietary considerations, particularly for new denture wearers. The conclusion highlights the role of prosthodontists in educating elderly patients about nutrition to combat prevalent deficiencies.

































































![Awareness of digital currency[1] (1).pptx](https://cdn.slidesharecdn.com/ss_thumbnails/awarenessofdigitalcurrency11-260125155504-b1badee4-thumbnail.jpg?width=640&height=640&fit=bounds)




