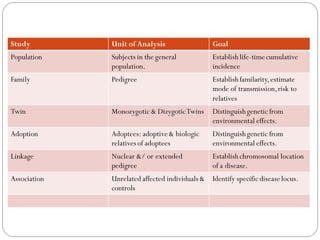
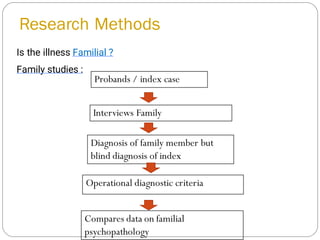
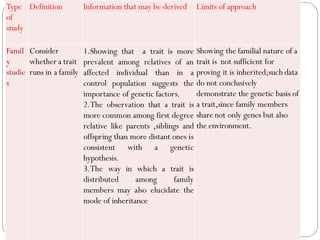
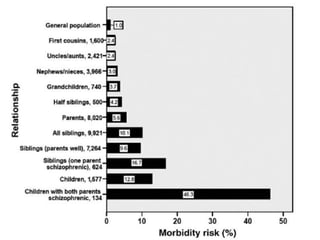
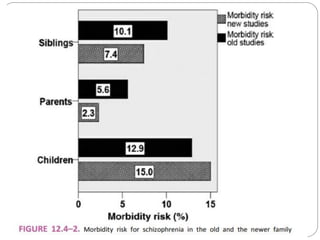
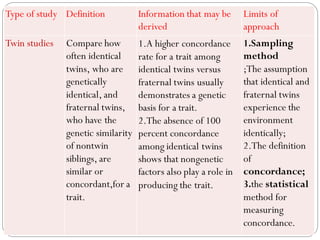
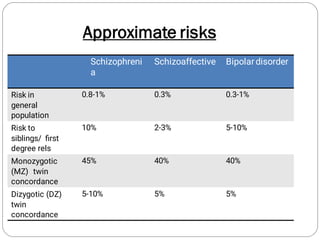
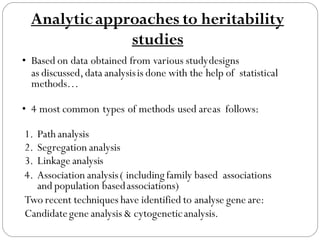
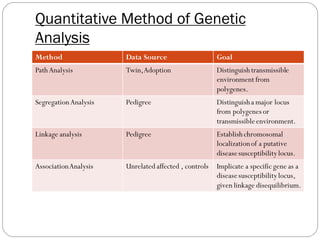
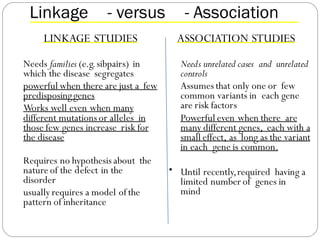
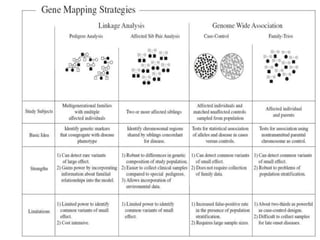
This document provides an overview of genetics in psychiatry. It begins with definitions of genetics and psychiatric genetics. It then discusses the history of genetics, basic genetics concepts like genes and genomes, and types of inheritance patterns like dominant, recessive, X-linked, and polygenic inheritance. The document reviews study designs used in psychiatric genetics research like family, twin, and adoption studies. It also discusses methods of genetic analysis including linkage analysis, association studies, and candidate gene studies. Overall, the document provides a comprehensive introduction to the field of psychiatric genetics.