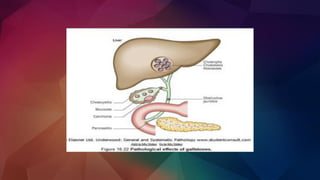
Gallstones are solid particles that form in the gallbladder, often composed of cholesterol or bilirubin. They can be asymptomatic or cause severe pain, known as biliary colic, typically in the upper right abdomen. Risk factors include obesity, diet, family history, and certain medical conditions. Treatment options range from watchful waiting for asymptomatic stones to surgical removal of the gallbladder (cholecystectomy) for symptomatic cases. Lifestyle changes and medications may also be recommended to manage symptoms and prevent recurrence.