Download as DOC, PPTX
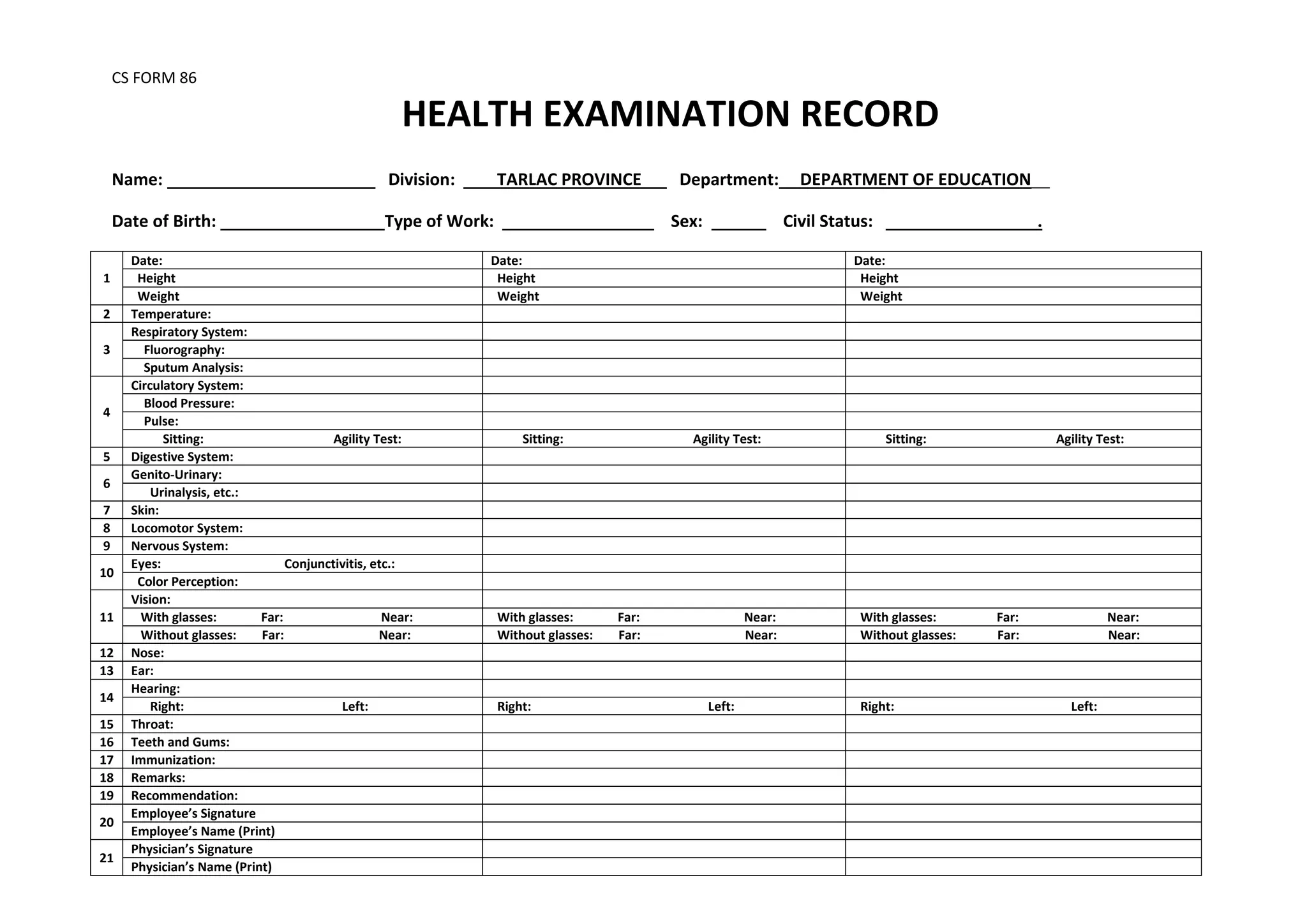

This document contains a health examination record for a civil servant. It includes sections to record personal details like name, date of birth, type of work, and civil status. It also includes sections to record measurements of height, weight, temperature, and assessments of various body systems like respiratory, circulatory, digestive, genitourinary, skin, locomotor, nervous, eyes, ears, nose, throat, teeth and gums. There are also sections to record vision testing results, hearing tests, immunization history, any remarks, physician recommendations, and signatures of the employee and examining physician.