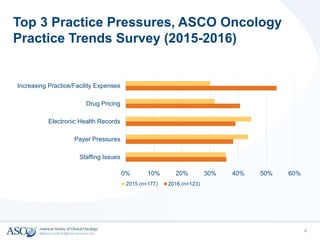
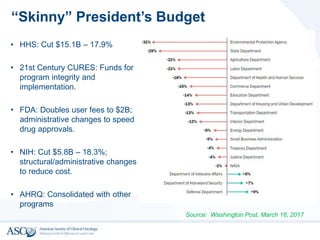
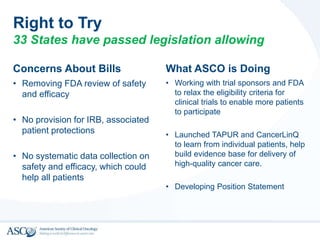
This document summarizes ASCO's policy priorities and outlook for 2017-2018. It discusses three main goals: pursuing affordable and high quality cancer care, supporting oncology providers, and advocating for cancer research funding. It also outlines top practice pressures like staffing and drug pricing. The document reviews the American Health Care Act and its potential impacts. It discusses other administration priorities around the budget, drug pricing, "Right to Try" legislation, and MACRA implementation. Finally, it notes that action is increasingly happening at the state level around issues like opioids, clinical pathways, and oral chemotherapy parity.