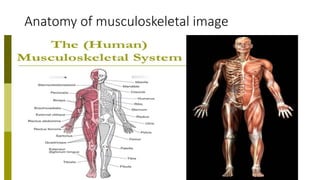
The document presents a comprehensive overview of musculoskeletal system examination techniques, including history-taking, observation, palpation, range of motion, and red flag assessments. It highlights the anatomy and function of various components like bones, muscles, tendons, and ligaments, as well as neurological aspects affecting motor control and pain perception. The document also outlines specific assessment methods for various joints and provides recommendations for imaging and laboratory investigations.