More Related Content

























Similar to Figure 8 Device Early Clinical Results




















More from W. Thomas McClellan, MD FACS


























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













Figure 8 Device Early Clinical Results
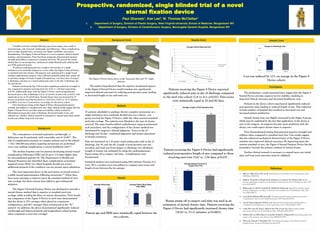
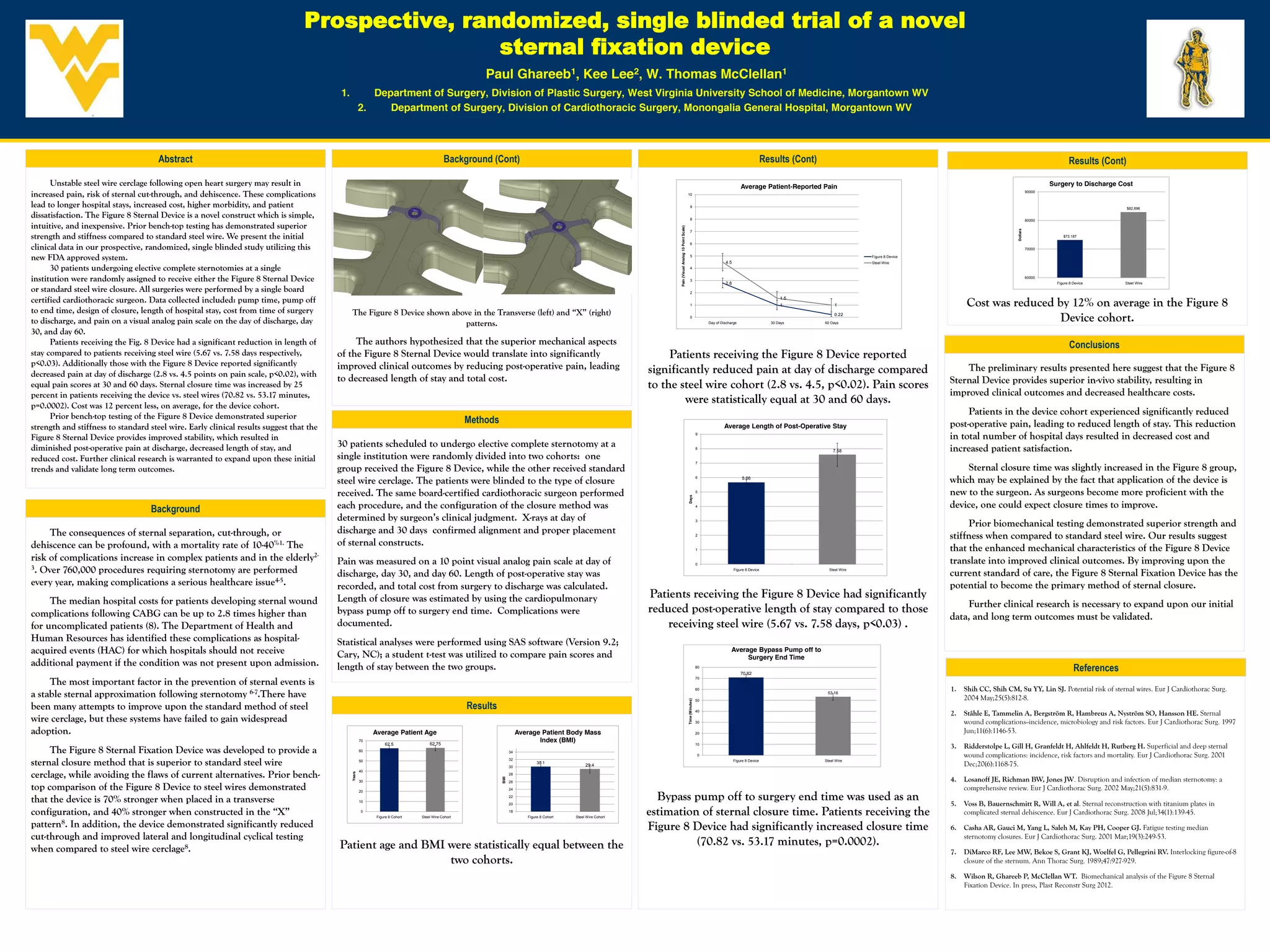
- 1. Prospective, randomized, singleblinded trial of a novel sternal fixation device Paul Ghareeb1, Kee Lee2, W. Thomas McClellan1 1. Department of Surgery, Division of Plastic Surgery, West Virginia University School of Medicine, Morgantown WV 2. Department of Surgery, Division of Cardiothoracic Surgery, Monongalia General Hospital, Morgantown WV Abstract Background (Cont) Results (Cont) Results (Cont) Unstable steel wire cerclage following open heart surgery may result in Average Patient-Reported Pain Surgery to Discharge Cost increased pain, risk of sternal cut-through, and dehiscence. These complications 10 90000 lead to longer hospital stays, increased cost, higher morbidity, and patient 9 $82,896 dissatisfaction. The Figure 8 Sternal Device is a novel construct which is simple, 8 80000 intuitive, and inexpensive. Prior bench-top testing has demonstrated superior Pain (Visual Analog 10 Point Scale) Dollars 7 strength and stiffness compared to standard steel wire. We present the initial $73,187 6 clinical data in our prospective, randomized, single blinded study utilizing this 70000 new FDA approved system. 5 4.5 Figure 8 Device Steel Wire 30 patients undergoing elective complete sternotomies at a single 4 institution were randomly assigned to receive either the Figure 8 Sternal Device 3 2.8 60000 Figure 8 Device Steel Wire or standard steel wire closure. All surgeries were performed by a single board 2 certified cardiothoracic surgeon. Data collected included: pump time, pump off 1 1.5 1 1 Cost was reduced by 12% on average in the Figure 8 to end time, design of closure, length of hospital stay, cost from time of surgery The Figure 8 Device shown above in the Transverse (left) and “X” (right) to discharge, and pain on a visual analog pain scale on the day of discharge, day patterns. 0 Day of Discharge 30 Days 0.22 60 Days Device cohort. 30, and day 60. Patients receiving the Fig. 8 Device had a significant reduction in length of The authors hypothesized that the superior mechanical aspects Conclusions stay compared to patients receiving steel wire (5.67 vs. 7.58 days respectively, of the Figure 8 Sternal Device would translate into significantly Patients receiving the Figure 8 Device reported p<0.03). Additionally those with the Figure 8 Device reported significantly improved clinical outcomes by reducing post-operative pain, leading significantly reduced pain at day of discharge compared The preliminary results presented here suggest that the Figure 8 decreased pain at day of discharge (2.8 vs. 4.5 points on pain scale, p<0.02), with to decreased length of stay and total cost. Sternal Device provides superior in-vivo stability, resulting in equal pain scores at 30 and 60 days. Sternal closure time was increased by 25 to the steel wire cohort (2.8 vs. 4.5, p<0.02). Pain scores percent in patients receiving the device vs. steel wires (70.82 vs. 53.17 minutes, improved clinical outcomes and decreased healthcare costs. p=0.0002). Cost was 12 percent less, on average, for the device cohort. were statistically equal at 30 and 60 days. Prior bench-top testing of the Figure 8 Device demonstrated superior Patients in the device cohort experienced significantly reduced Methods post-operative pain, leading to reduced length of stay. This reduction strength and stiffness to standard steel wire. Early clinical results suggest that the Average Length of Post-Operative Stay Figure 8 Sternal Device provides improved stability, which resulted in 9 in total number of hospital days resulted in decreased cost and diminished post-operative pain at discharge, decreased length of stay, and 30 patients scheduled to undergo elective complete sternotomy at a 8 increased patient satisfaction. 7.58 reduced cost. Further clinical research is warranted to expand upon these initial single institution were randomly divided into two cohorts: one 7 trends and validate long term outcomes. group received the Figure 8 Device, while the other received standard Sternal closure time was slightly increased in the Figure 8 group, steel wire cerclage. The patients were blinded to the type of closure 6 5.66 which may be explained by the fact that application of the device is received. The same board-certified cardiothoracic surgeon performed 5 new to the surgeon. As surgeons become more proficient with the Days Background each procedure, and the configuration of the closure method was 4 device, one could expect closure times to improve. determined by surgeon’s clinical judgment. X-rays at day of 3 Prior biomechanical testing demonstrated superior strength and The consequences of sternal separation, cut-through, or discharge and 30 days confirmed alignment and proper placement 2 stiffness when compared to standard steel wire. Our results suggest dehiscence can be profound, with a mortality rate of 10-40%1. The of sternal constructs. 1 that the enhanced mechanical characteristics of the Figure 8 Device risk of complications increase in complex patients and in the elderly2- Pain was measured on a 10 point visual analog pain scale at day of 0 translate into improved clinical outcomes. By improving upon the 3. Over 760,000 procedures requiring sternotomy are performed discharge, day 30, and day 60. Length of post-operative stay was Figure 8 Device Steel Wire current standard of care, the Figure 8 Sternal Fixation Device has the every year, making complications a serious healthcare issue4-5. recorded, and total cost from surgery to discharge was calculated. potential to become the primary method of sternal closure. Length of closure was estimated by using the cardiopulmonary Patients receiving the Figure 8 Device had significantly The median hospital costs for patients developing sternal wound Further clinical research is necessary to expand upon our initial complications following CABG can be up to 2.8 times higher than bypass pump off to surgery end time. Complications were reduced post-operative length of stay compared to those data, and long term outcomes must be validated. for uncomplicated patients (8). The Department of Health and documented. receiving steel wire (5.67 vs. 7.58 days, p<0.03) . Human Resources has identified these complications as hospital- Statistical analyses were performed using SAS software (Version 9.2; acquired events (HAC) for which hospitals should not receive Cary, NC); a student t-test was utilized to compare pain scores and Average Bypass Pump off to Surgery End Time additional payment if the condition was not present upon admission. length of stay between the two groups. 80 70.82 References The most important factor in the prevention of sternal events is 70 60 1. Shih CC, Shih CM, Su YY, Lin SJ. Potential risk of sternal wires. Eur J Cardiothorac Surg. a stable sternal approximation following sternotomy 6-7.There have 50 53.16 2004 May;25(5):812-8. Time (Minutes) been many attempts to improve upon the standard method of steel Results 40 2. Ståhle E, Tammelin A, Bergström R, Hambreus A, Nyström SO, Hansson HE. Sternal wire cerclage, but these systems have failed to gain widespread 30 wound complications--incidence, microbiology and risk factors. Eur J Cardiothorac Surg. 1997 adoption. Average Patient Age Average Patient Body Mass 20 Jun;11(6):1146-53. 70 62.75 Index (BMI) 62.5 10 3. Ridderstolpe L, Gill H, Granfeldt H, Ahlfeldt H, Rutberg H. Superficial and deep sternal The Figure 8 Sternal Fixation Device was developed to provide a 60 34 0 wound complications: incidence, risk factors and mortality. Eur J Cardiothorac Surg. 2001 sternal closure method that is superior to standard steel wire 50 32 30 30.1 29.4 Figure 8 Device Steel Wire Dec;20(6):1168-75. cerclage, while avoiding the flaws of current alternatives. Prior bench- 40 Years 28 4. Losanoff JE, Richman BW, Jones JW. Disruption and infection of median sternotomy: a BMI 30 26 top comparison of the Figure 8 Device to steel wires demonstrated 24 comprehensive review. Eur J Cardiothorac Surg. 2002 May;21(5):831-9. Bypass pump off to surgery end time was used as an 20 that the device is 70% stronger when placed in a transverse 10 22 20 5. Voss B, Bauernschmitt R, Will A, et al. Sternal reconstruction with titanium plates in configuration, and 40% stronger when constructed in the “X” 0 Figure 8 Cohort Steel Wire Cohort 18 Figure 8 Cohort Steel Wire Cohort estimation of sternal closure time. Patients receiving the complicated sternal dehiscence. Eur J Cardiothorac Surg. 2008 Jul;34(1):139-45. pattern8. In addition, the device demonstrated significantly reduced Figure 8 Device had significantly increased closure time 6. Casha AR, Gauci M, Yang L, Saleh M, Kay PH, Cooper GJ. Fatigue testing median cut-through and improved lateral and longitudinal cyclical testing sternotomy closures. Eur J Cardiothorac Surg. 2001 Mar;19(3):249-53. Patient age and BMI were statistically equal between the (70.82 vs. 53.17 minutes, p=0.0002). when compared to steel wire cerclage8. 7. DiMarco RF, Lee MW, Bekoe S, Grant KJ, Woelfel G, Pellegrini RV. Interlocking figure-of-8 two cohorts. closure of the sternum. Ann Thorac Surg. 1989;47:927-929. 8. Wilson R, Ghareeb P, McClellan WT. Biomechanical analysis of the Figure 8 Sternal Fixation Device. In press, Plast Reconstr Surg 2012.