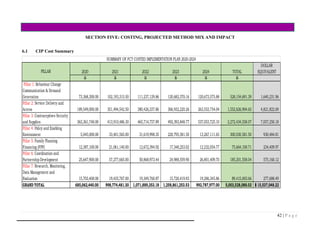
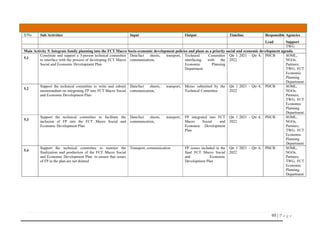
The document outlines the Costed Implementation Plan (CIP) for Family Planning in the Federal Capital Territory (FCT) of Nigeria from 2020 to 2024, aiming to enhance access to family planning services to reduce maternal and child mortality. It highlights the need for multi-sector collaboration to achieve a contraceptive prevalence rate goal of 30%, ultimately preventing significant numbers of unintended pregnancies and maternal deaths. The plan emphasizes the roles of various stakeholders, the importance of policy development, financing, and effective monitoring to ensure successful implementation.






![x | P a g e
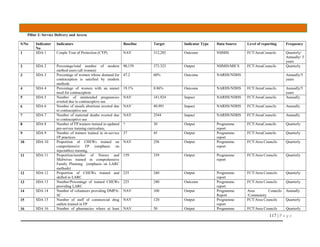
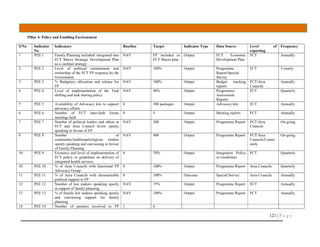
LIST OF CONTRIBUTORS
S/N NAMES Position & Organisation Thematic Area Worked
1 Dr. Ndaeyo Iwot Ag ES,FCT PHCB Family Planning Financing
2 Dr. RuqayyatWamako Director PHCB Policy & Enabling Environment
3 Mrs. Momoh Mariam Family Planning Coordinator Coordination and Partnership
4 Muhammad A. Lawal Director EPRS Family Planning Financing
5 Mrs. Ajoke Alao Data Officer[Family Planning] Contraceptives & Supplies
6 Evelyn Max Egba Npower FP Coordinating Unit Family Planning Financing
7 Victoria Aleoghena Education Secretariat Family Planning Financing
8 Fatigun Olusegun FCT/UNFPA Programme Coordinator Policy & Enabling Environment
9 Dr. Dan-Gadzama M and E Officer PHCB Research, Monitoring & Evaluation
10 Mrs. Kanu Felicia Provider, Luingi Barracks Service Delivery and Access
11 Mrs. Daghuje Florence School of Midwifery, Gwagwalada Service Delivery and Access
12 Mrs. Attah Elizabeth Deputy FP Coordinator Coordination and Partnership
13 Iyabo Balogun Area council FP/RH Coordinator Research, Monitoring & Evaluation
14 Mrs. Eniola Awoniyi Provider Family Health Clinic Area 2 Service Delivery and Access
15 Mosunmola Adefila Npower FP Coordinating Unit BCC/Demand Generation
16 Pharm Peter Ibrahim Pharmacist PHCB Policy & Enabling Environment
17 Peter Alfa Budget Officer PHCB Policy & Enabling Environment
18 Mrs. Carol Ibrahim PRS Family Planning Financing
19 Hajia Halima Gero LMCU Coordinator Contraceptives & Supplies
20 Mrs. Munirat Usman Provider Nyanya General Hospital Family Planning Financing
21 Dr. M.O.D Abonyi Chairman AGPMPN Coordination and Partnership
22 Dr. Joachim Chijide FP/RHCS Specialist, UNFPA Research, Monitoring & Evaluation
23 Dr. Ismail A. Mohammed SHOPS Plus USAID Coordination and Partnership
24 Shafa Ahmed Salihu Community Health Practitioner BCC/Demand Generation
25 HakeematAliyu NTA BCC/Demand Generation
26 Miss Rita Anene Program Officer, PPFN Service Delivery and Access
27 Dr. Isah Vasta Director PRS PHCB Research, Monitoring & Evaluation
28 Mr Eze Josephat Secretary AGPNP Family Planning Financing
29 Omolewa Yemisi Education Secretary BCC/Demand Generation
30 Hajara Onubaiye Family Planning Coordinating Unit Policy & Enabling Environment
31 Emilene Anakhuekha FCT Focal Person, UNFPA Coordination and Partnership
32 Dr. Hadley Ikwe FP Analyst, UNFPA BCC/Demand Generation](https://image.slidesharecdn.com/fctfamilyplanningcostedimplementationplan-201227135540/85/FCT-Family-Planning-Costed-implementation-Plan-10-320.jpg)

























































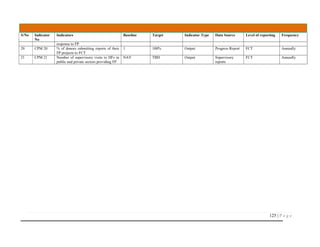
![115 | P a g e
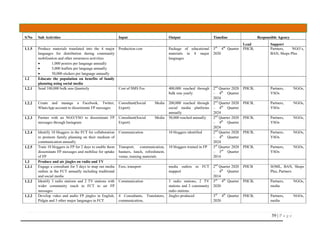
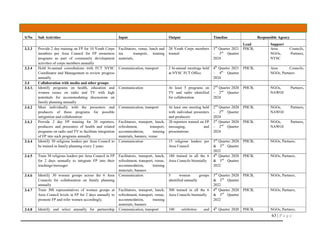
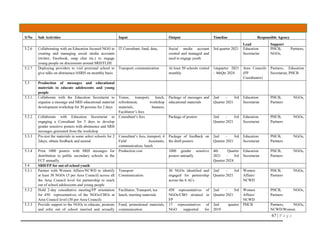
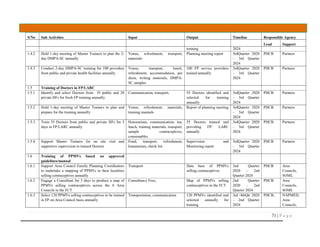
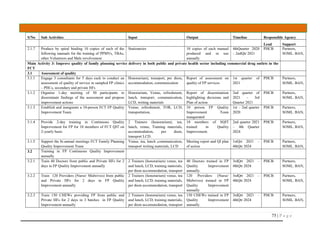
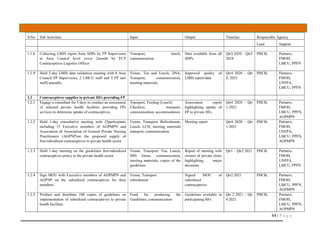
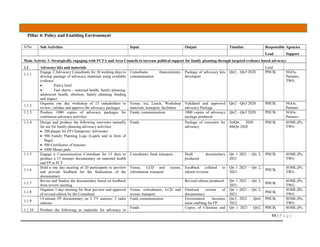
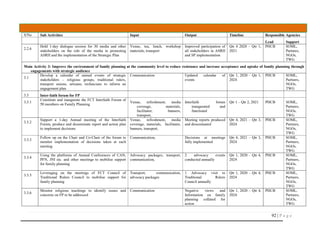
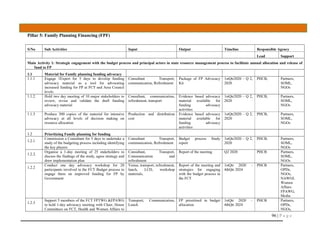
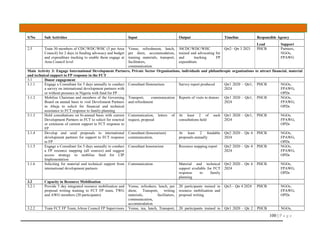
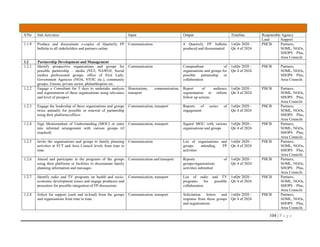
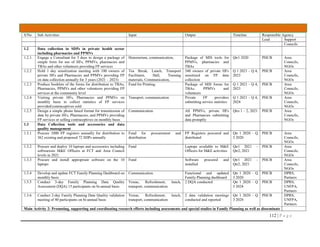
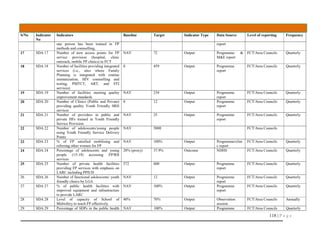
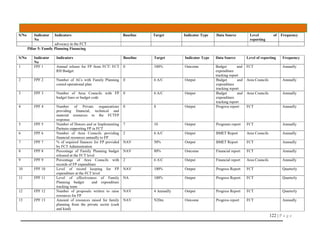
ANNEX 2: CIP Results Framework
S/No Indicator
No
Indicators Baseline Target Indicator
Type
Data Source Level of
reporting
Frequency
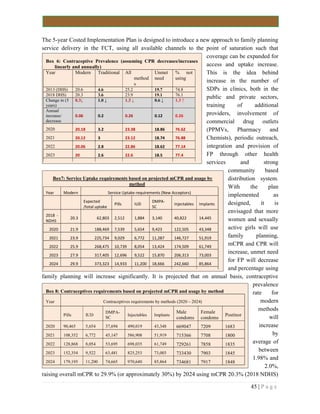
CIP 1 Contraceptive Prevalence rate (All methods) 23.9% 33.5 (FCT)
CIP 2 Modern contraceptive prevalence (mCPR] 20.3% 29.9% (for FCT) Impact NDHS/MICS State Annually/5 years
CIP 3 Contraceptive continuation rates (Revisit) Impact Special Studies FCT/Area
Councils
Annually/5 years
CIP 4 Maternal Mortality Ratio NAV TBD Impact NDHS/MICS State Annually/5 years
CIP 5 Total Fertility Rate 4.3 3.8 Impact NDHS/MICS State Annually/5 years
CIP 6 Preferred Fertility 3.8 3.8 Impact NDHS/MICS State Annually/5years
CIP 7 Unmet Need for Family Planning 19.1 8.86 Impact NDHS/MICS State Annually/5 years
CIP 8 Adolescent Fertility/Teenage Motherhood 39 30 Impact NDHS/MICS State Annually/5 years
CIP 9 Adolescent/Sexually Active Unmarried Women
Contraceptive Rate (mCPR)
28% 37.9 Impact NDHS/MICS State Annually/5 years
CIP 10 Contraceptive Prevalence Rate (Traditional) 3.6 0.4 Impact NDHS/MICS State Annually/5 years
Pillar 1: Behaviour Change Communication/Demand Generation
BDG 1 Percentage of Women and Men of Reproductive
Age who have heard about (at least three methods
of) Family Planning
NAV 80% Outcome NDHS/NARHS
/ MICS
FCT Annually/5 years
BDG 2 Percentage of the population who know of at least
one source of modern contraceptive services
NAV 80% Outcome NDHS/NARHS
/ MICS
FCT 5 years/Annually
BDG 3 Percentage of men and women with favourable
attitude towards FP, its acceptance and use
NAV 80% Outcome NDHS/NARHS
/ MICS
FCT 5 years/Annually
BDG 4 Number of FP champions actively mobilising
support for FP in FCT
NAV 200 Output Programs report FCT/Area
Councils
Quarterly
BDG 5 Number of notable community/religious leaders
who have spoken in favour and mobilising for FP
NAV 400 Outcome Programs report FCT/Area
Councils
Quarterly
BDG 6 % of schools implementing FLHE according to
approved national guidelines
NAV 70% Output Programs report FCT/Area
Councils
Quarterly
BDG 7 % of teachers trained and teaching FLHE in public
Schools
NAV 50% Output Programs report FCT/Area
Councils
Quarterly
BDG 8 Number of students trained and operating as peer
educators in FLHE, educating and referring their
peers
NAV TBD Output Programs report FCT/Area
Councils
Quarterly
9 BDG 9 Percentage of women who make FP decisions alone 31%/58.5 40%/70% Outcome NDHS/NARHS FCT 5 years/Annually](https://image.slidesharecdn.com/fctfamilyplanningcostedimplementationplan-201227135540/85/FCT-Family-Planning-Costed-implementation-Plan-128-320.jpg)















![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)

![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)
















