Download to read offline
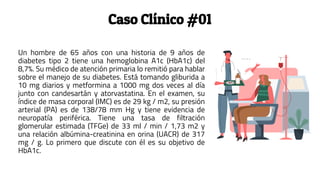
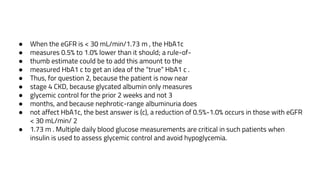
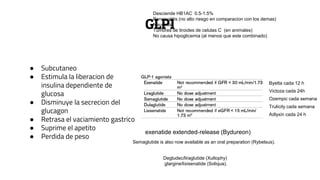
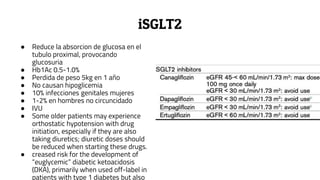





































This document provides guidance on managing diabetes in patients with chronic kidney disease. It discusses epidemiology and the importance of glycemic control in slowing kidney disease progression. A case study is presented of a 65-year-old man with type 2 diabetes and stage 3 CKD, and appropriate HbA1c goals and measurement considerations are reviewed. Options for antihyperglycemic agents in CKD, including risks and benefits, are covered. Acute kidney injury is defined as a sudden reduction in renal function.










































![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)










