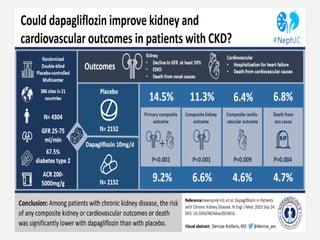
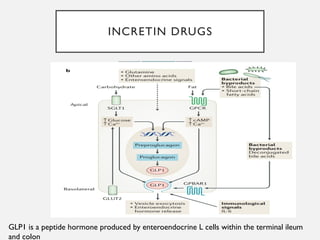
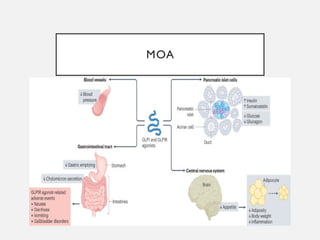
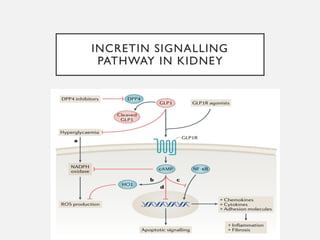
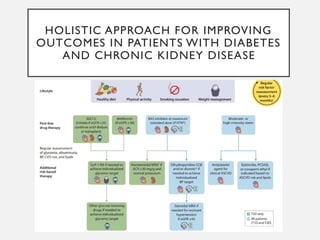
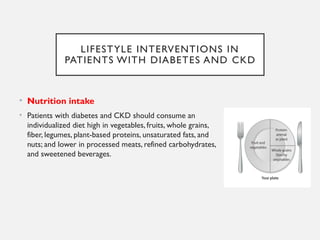
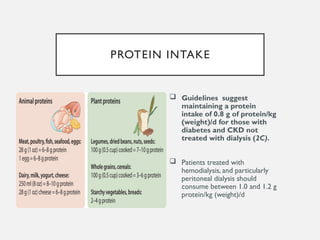
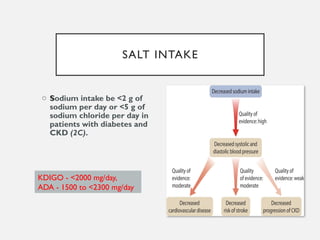
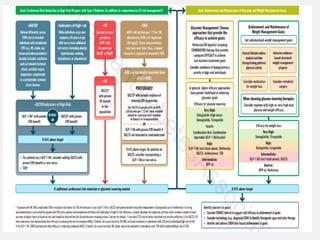
The document discusses the management of diabetic nephropathy through a holistic approach, emphasizing lifestyle interventions such as individualized nutrition, protein intake, salt restriction, and smoking cessation. It highlights the importance of glycemic control, weight management, and appropriate medication use, including SGLT-2 inhibitors and GLP-1 receptor agonists, while addressing blood pressure and lipid management. Additionally, it reviews the role of antithrombotic therapy in reducing cardiovascular risks in patients with diabetes and chronic kidney disease.


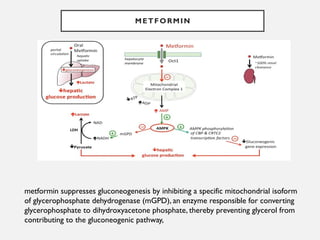
![METFORMIN IS CONTRAINDICATED IN PATIENTS WITH
FACTORS PREDISPOSING TO LACTIC ACIDOSIS.
Impaired kidney function (estimated glomerular filtration rate [eGFR]
Concurrent active or progressive severe liver disease
Active alcohol abuse
Unstable or acute heart failure at risk of hypoperfusion
Past history of lactic acidosis during metformin therapy
Decreased tissue perfusion or hemodynamic instability due to infection or other causes](https://image.slidesharecdn.com/diabeticnephropathy-management-241026091934-3e77e050/85/DIABETIC-NEPHROPATHY-management-pptx-recent-23-320.jpg)