Downloaded 15 times

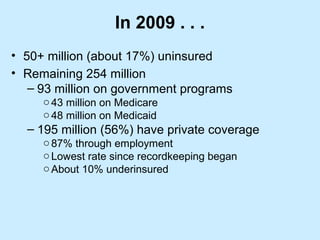
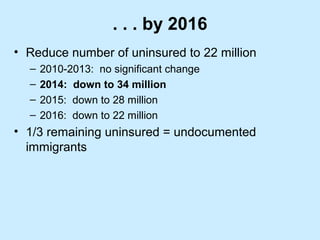

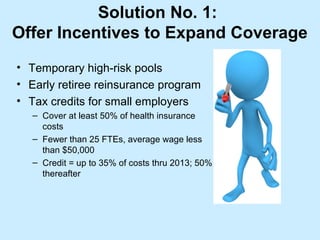
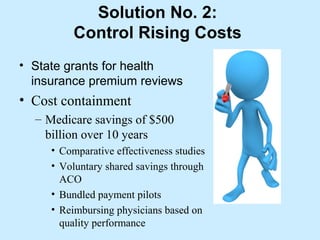









The document discusses the Affordable Care Act (ACA), highlighting its significance as a comprehensive healthcare reform aimed at expanding insurance coverage and controlling costs. Key features include the establishment of health insurance exchanges, individual mandates, Medicaid expansion, and measures to regulate health plan coverage. It also addresses the impact of ACA on uninsured rates, hospital services, and the future of healthcare delivery systems in the U.S.



























































![[HOW TO] Create High Performance Emergency Departments](https://cdn.slidesharecdn.com/ss_thumbnails/edperformancewhitepaper-140110130313-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)























