The document discusses the challenges healthcare providers face in educating patients due to various barriers such as literacy, culture, and physiological factors. It emphasizes the importance of assessing patients' learning needs and adapting teaching techniques to ensure effective communication. The article highlights the different learning styles and the significance of cultural competency in enhancing patient education and outcomes.

![by health care professionals to ensure that the pa-
tient understands the information given to him or
her. Barriers that inhibit patient education are liter-
acy, language, culture, and physiological obstacles.
Assessing and evaluating the learning needs of
the patient are essential before planning and im-
plementation of an educational plan. Presenting
a well-formulated plan will increase the likelihood
of a successful recovery for the patient. In this
article, barriers will be dissected and strategies
examined to determine what will best suit the edu-
cational needs of the patient.
S, BSN, RN, CPAN, is a PACU Clinical Edu-
enant Hospital, Chicago, IL.
st: None to report.
ondence to Linda Beagley, Swedish Cove-
40 N. California Ave, Chicago, IL 60625;
[email protected]
rican Society of PeriAnesthesia Nurses
00](https://image.slidesharecdn.com/educatingpatientsunderstandingbarrierslearningstyles-230108072755-9543459f/85/Educating-Patients-Understanding-Barriers-Learning-Styles-docx-3-320.jpg)
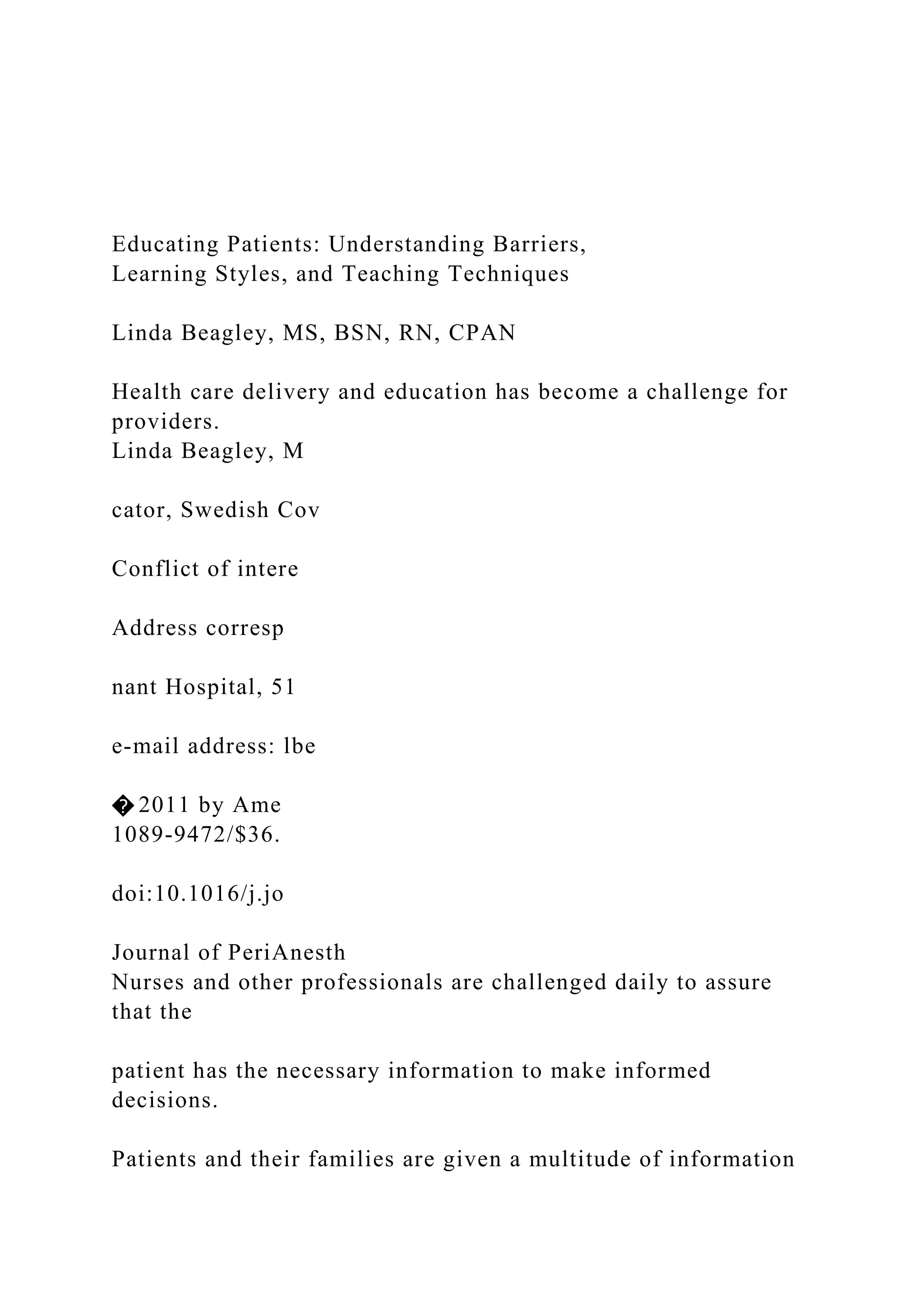
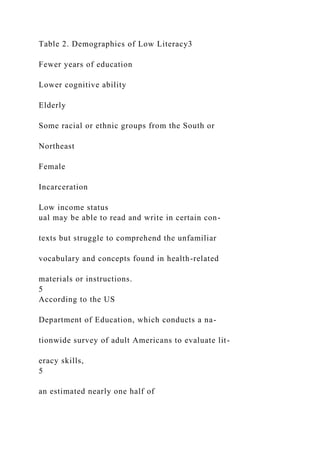
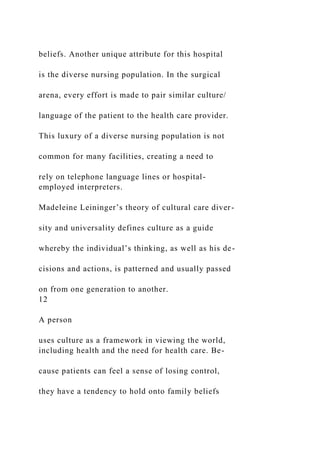
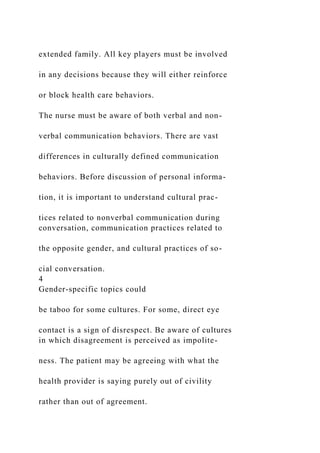
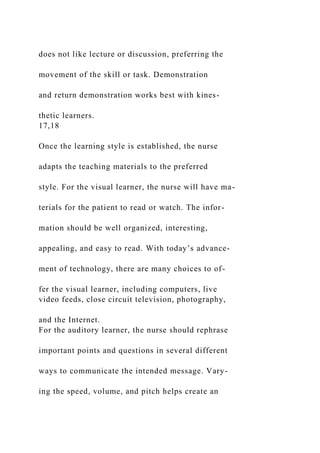
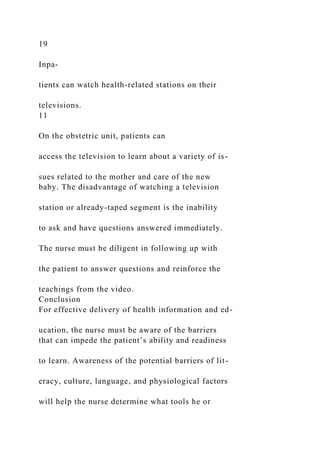
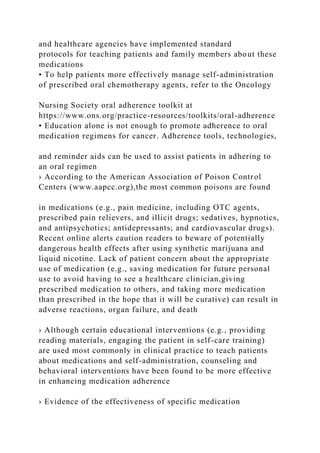
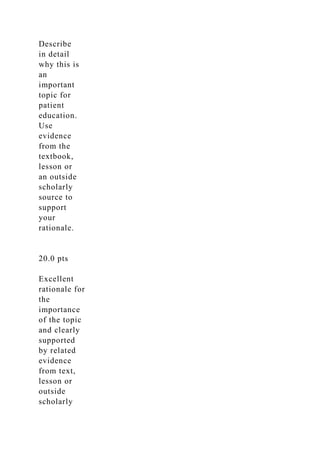
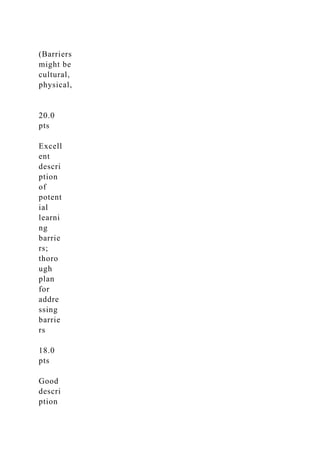
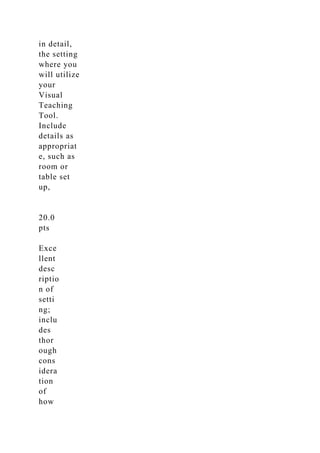
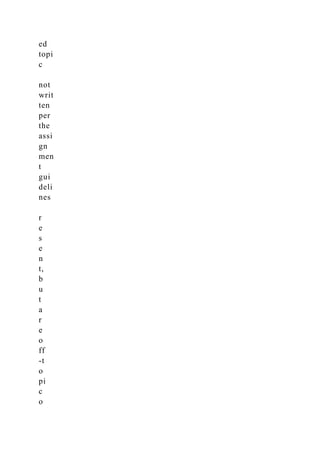
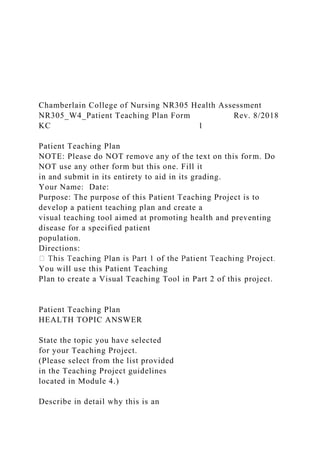
![a growing reservoir of knowledge, followed by
a readiness to learn, which increasingly is oriented
towards developmental tasks related to social roles
with immediate application of their new knowl-
edge. Knowles’ final assumption reflects the moti-
vation of learning as moving from external to
internal.
1,2
Table 1 compares and summarizes
Knowles’ assumption regarding the adult (andra-
gogy) and the child (pedagogy) learner.
331
mailto:[email protected]
http://dx.doi.org/10.1016/j.jopan.2011.06.002
Table 1. Assumptions Differences of Pedagogy and
Andragogy1,2
Assumptions Pedagogy Andragogy
Self-concept Dependency Self-directed
Experience Happens to learner Rich resource
Readiness Biologic and academic development Evolving social](https://image.slidesharecdn.com/educatingpatientsunderstandingbarrierslearningstyles-230108072755-9543459f/85/Educating-Patients-Understanding-Barriers-Learning-Styles-docx-5-320.jpg)
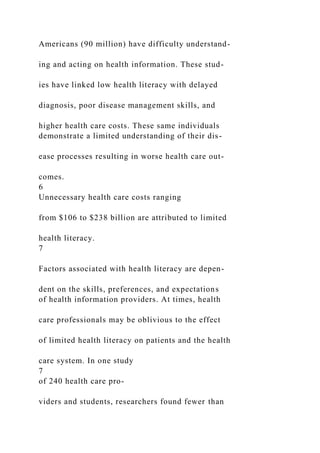



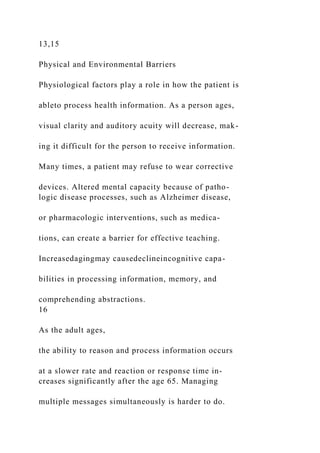


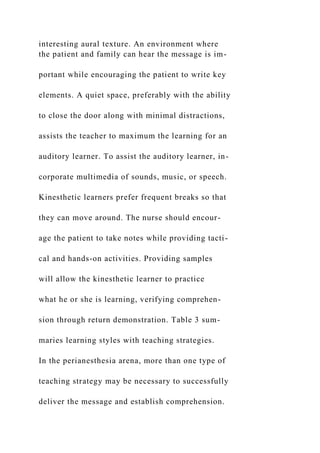

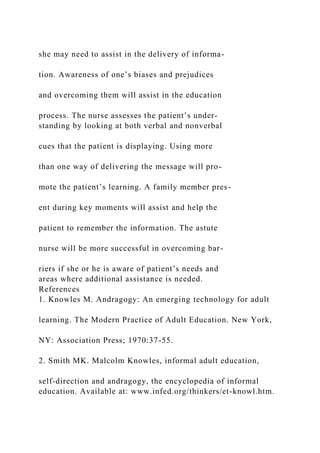












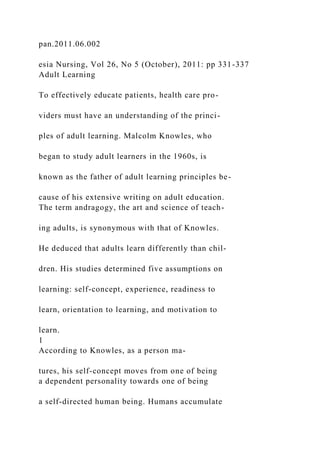
![family members or caregivers are available to support the
patient in learning
› Implement the patient education plan
• Discuss and set mutually achievable goals for learning about
medication self-administration with the patient
–Anticipate a planned approach to teaching and learning, but be
prepared to be flexible and individualize information based
on the patient’s changing needs and desires
• Emphasize the name, dose, route, timing, purpose, and adverse
effects of each medication, and educate about safety
concerns related to medication self-administration
–Make the education situation as realistic as possible; if
feasible, schedule home visits to coincide with the patient’s
medication self-administration times
–Allow sufficient time for the patient to practice skills and talk
about any concerns
–If the patient is not able to safely administer his/her
medication regimen, arrange for family members or other
caregivers
to support the patient as needed
• Promote collaborative partnerships between the patient and
members of the healthcare team to achieve the highest levels of
medication adherence
–Use open-ended requests that allow the patient to explain or
demonstrate and that enable the healthcare provider to verify
the patient’s understanding (e.g., “Tell me [or show me] how
you take your medication”)
–Ask specific questions about the patient’s medication regimen](https://image.slidesharecdn.com/educatingpatientsunderstandingbarrierslearningstyles-230108072755-9543459f/85/Educating-Patients-Understanding-Barriers-Learning-Styles-docx-53-320.jpg)


















































![Elements of Critical Thinking [WLOs 2, 3, 4] [CLOs 2, 3, 4]P.docx](https://cdn.slidesharecdn.com/ss_thumbnails/elementsofcriticalthinkingwlos234clos234p-230108072818-bdaff573-thumbnail.jpg?width=640&height=640&fit=bounds)



























