ECG - 1
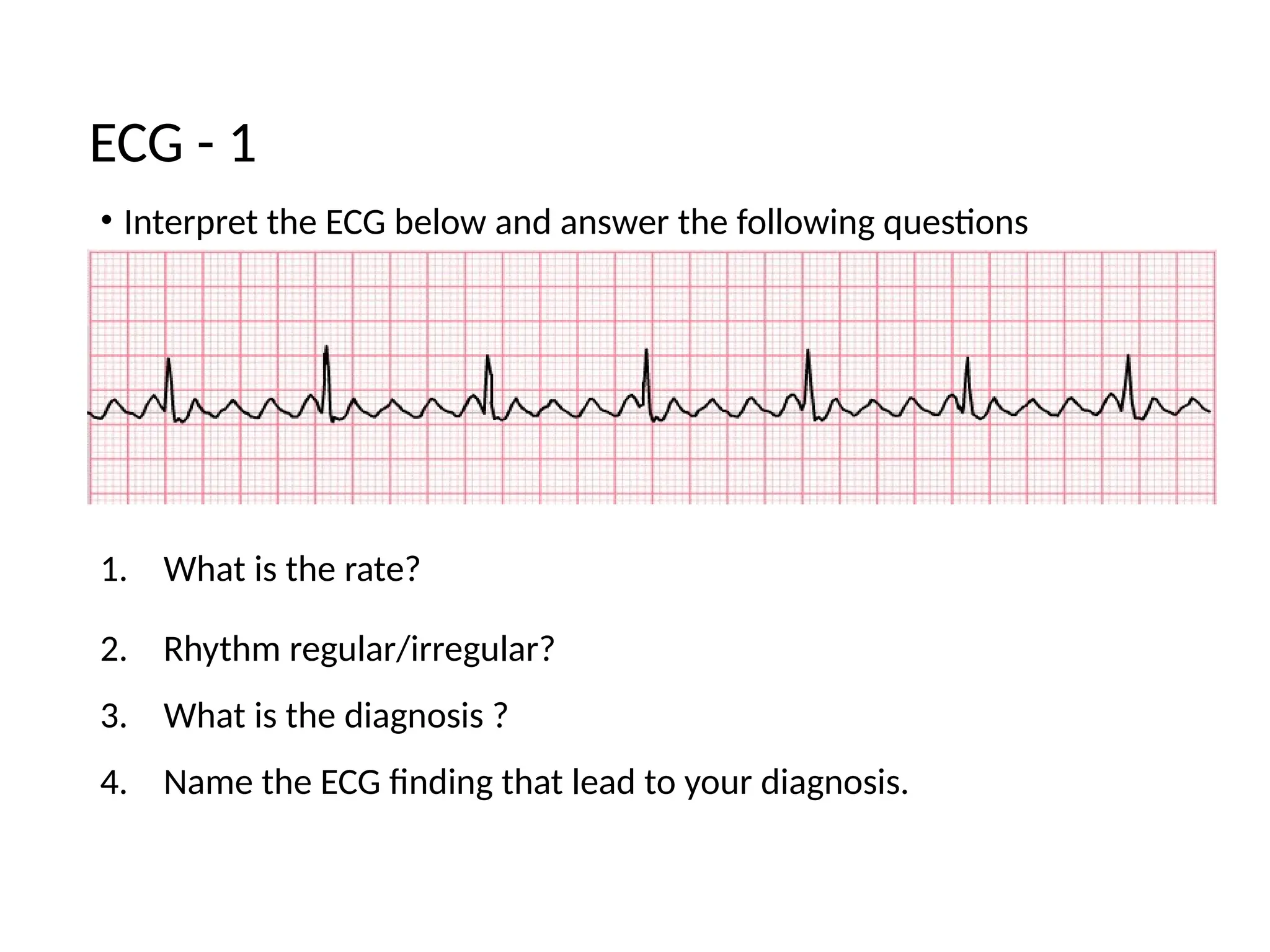
•Interpret the ECG below and answer the following questions
1. What is the rate?
2. Rhythm regular/irregular?
3. What is the diagnosis ?
4. Name the ECG finding that lead to your diagnosis.
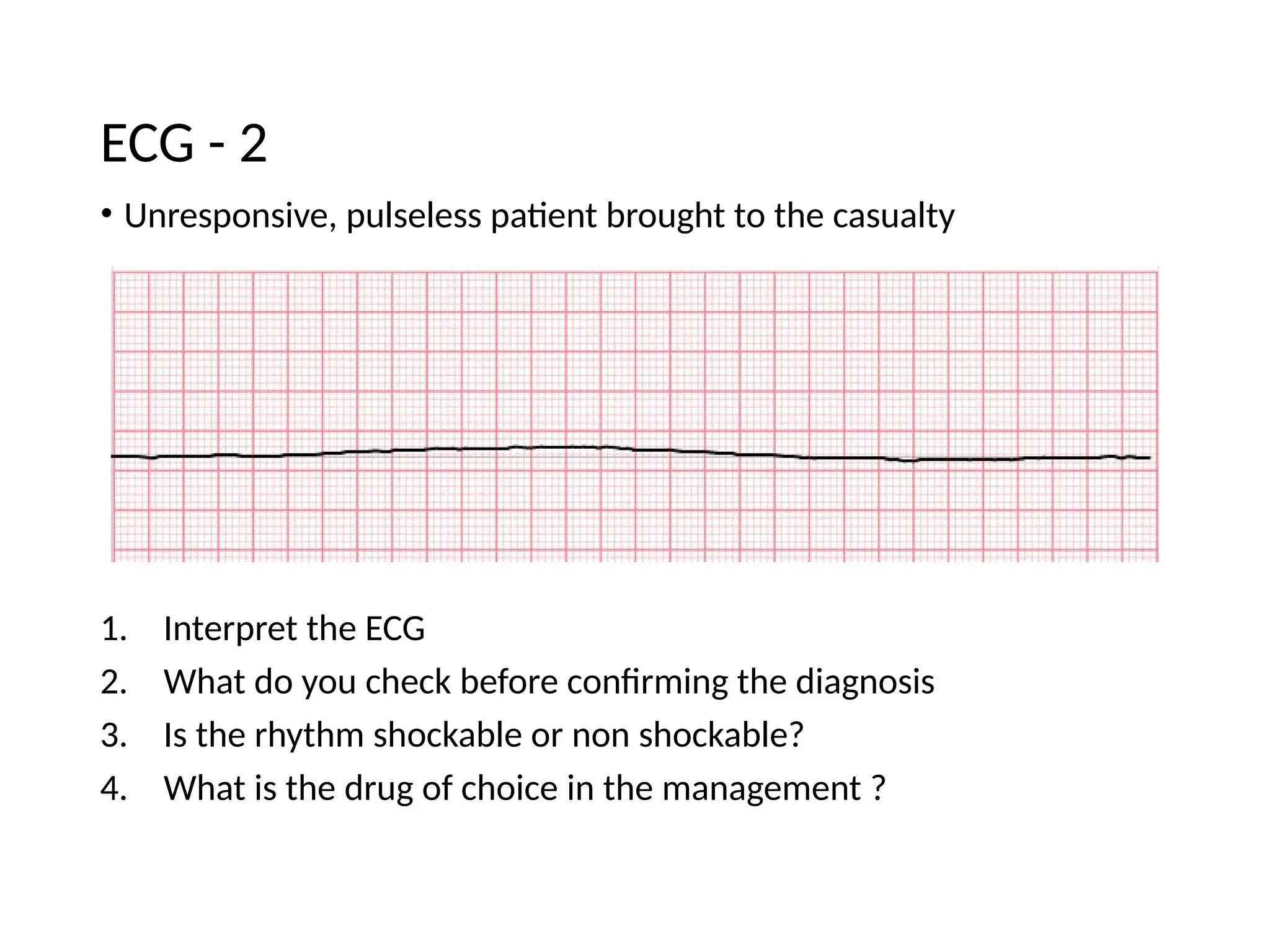
• Unresponsive, pulselesspatient brought to the casualty
1. Interpret the ECG
2. What do you check before confirming the diagnosis
3. Is the rhythm shockable or non shockable?
4. What is the drug of choice in the management ?
ECG - 2
5.
ECG 2
1. Asystole
2.Check the leads, augment the ECG
3. Non-shockable
4. adrenaline
6.
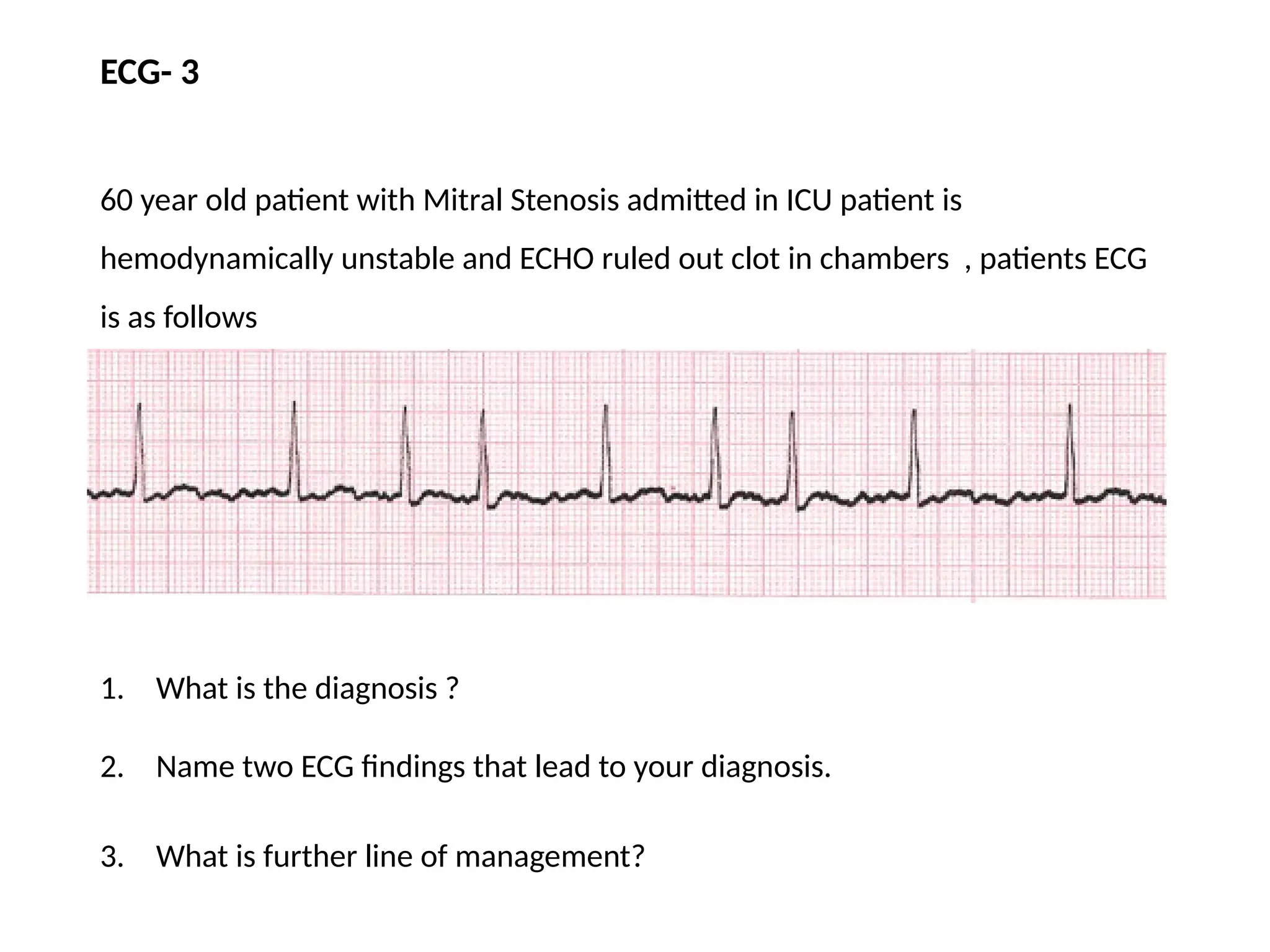
ECG- 3
60 yearold patient with Mitral Stenosis admitted in ICU patient is
hemodynamically unstable and ECHO ruled out clot in chambers , patients ECG
is as follows
1. What is the diagnosis ?
2. Name two ECG findings that lead to your diagnosis.
3. What is further line of management?
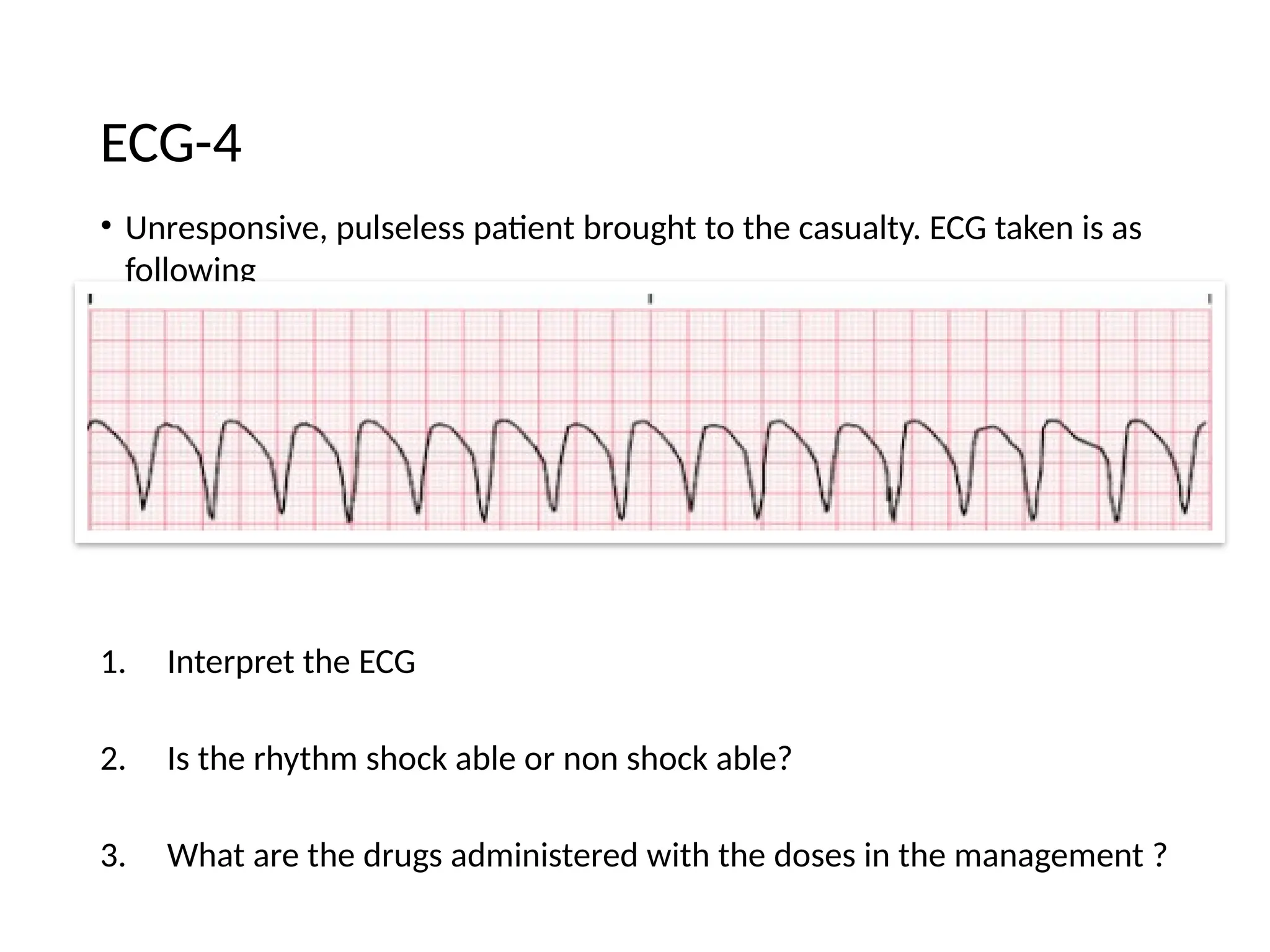
• Unresponsive, pulselesspatient brought to the casualty. ECG taken is as
following
1. Interpret the ECG
2. Is the rhythm shock able or non shock able?
3. What are the drugs administered with the doses in the management ?
ECG-4
9.
ECG - 4
•Ventricular tachycardia
• Shockable rhythm
• After 2nd shock administer Epinephrine 1 mg ,
• After 3rd shock Amiodarone 300mg first dose /Lignocaine 1-
1.5mg/kg
• After 5th schock 150mg 2nd
dose
10.
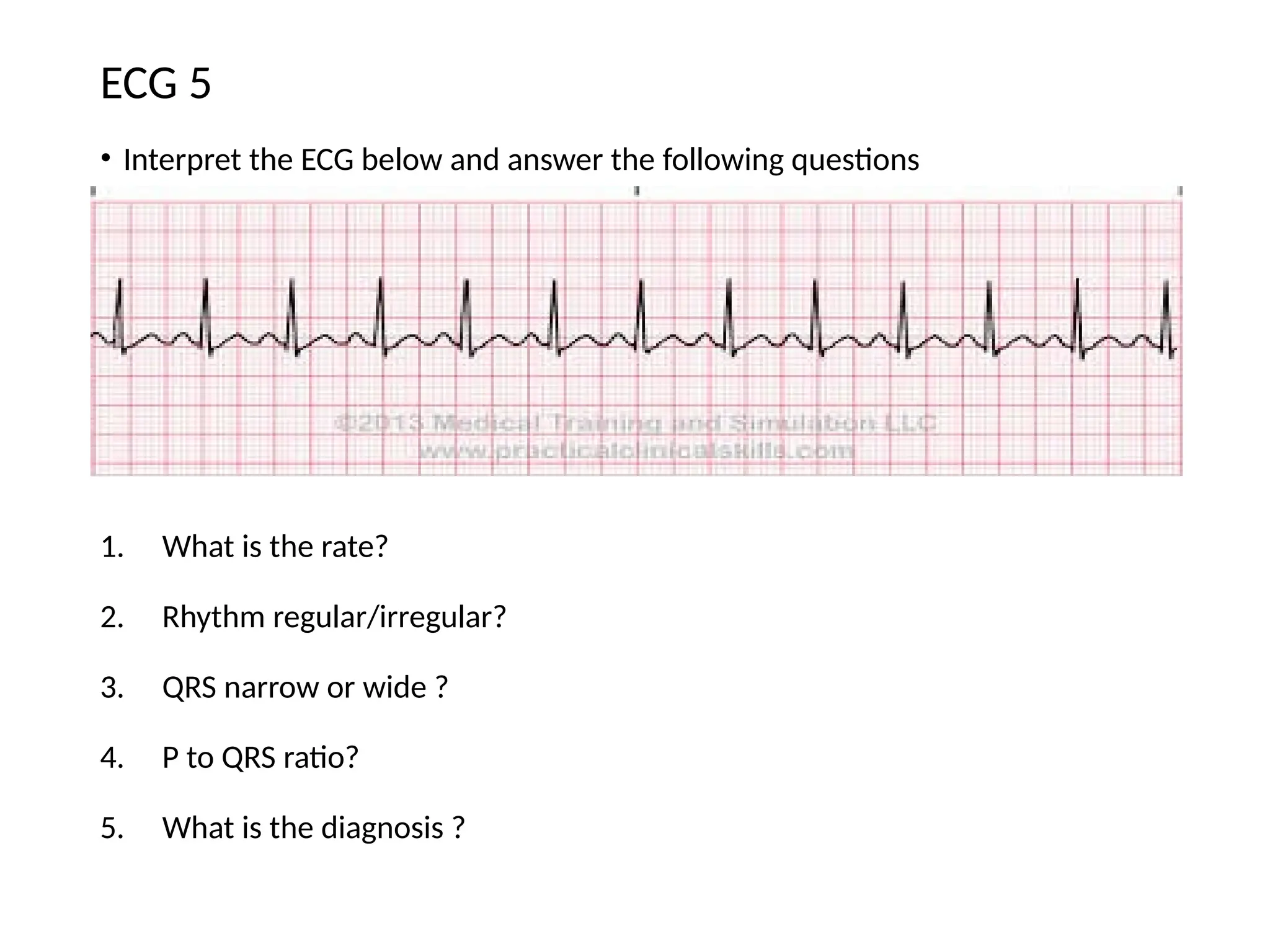
• Interpret theECG below and answer the following questions
1. What is the rate?
2. Rhythm regular/irregular?
3. QRS narrow or wide ?
4. P to QRS ratio?
5. What is the diagnosis ?
ECG 5
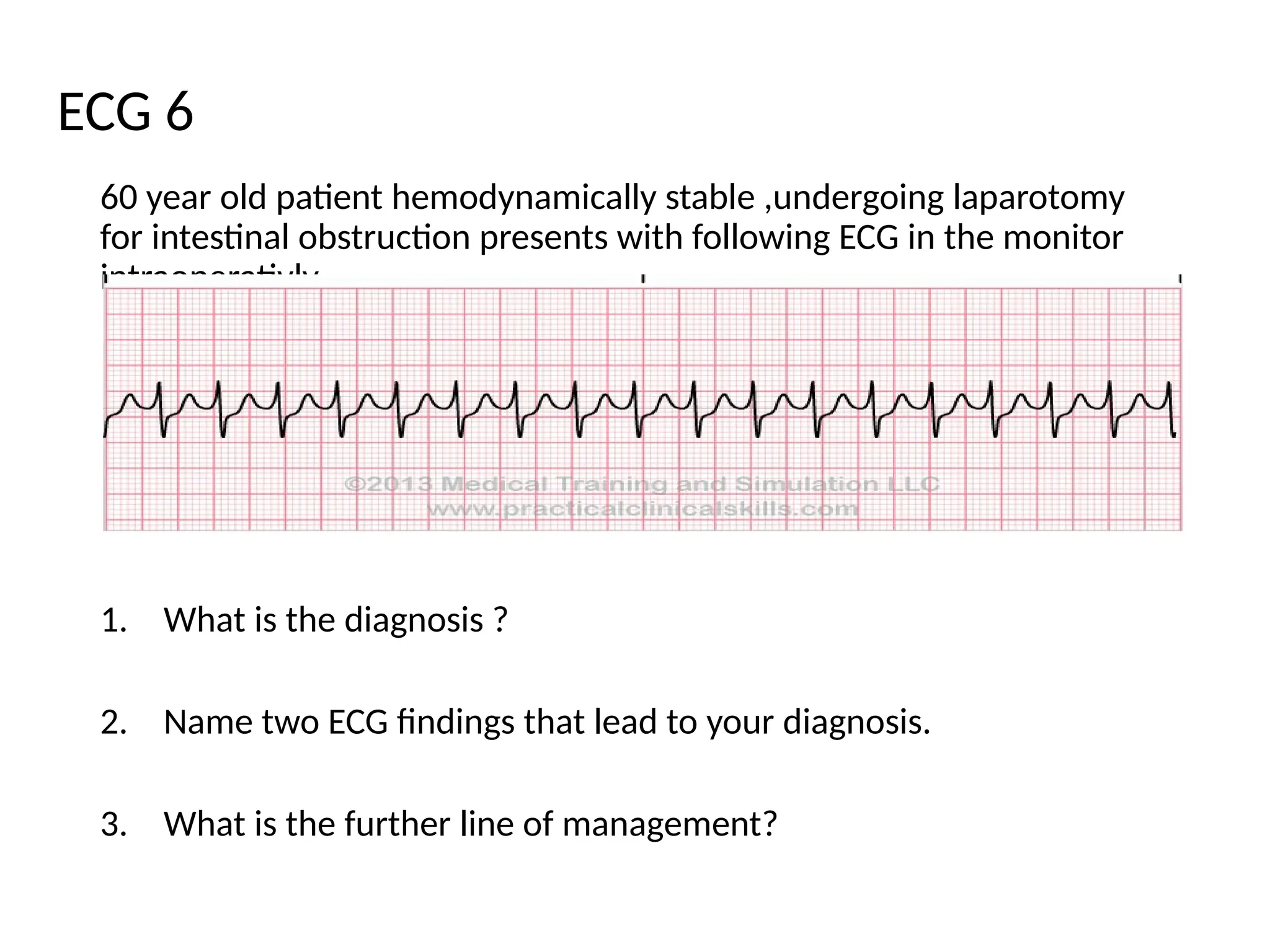
60 year oldpatient hemodynamically stable ,undergoing laparotomy
for intestinal obstruction presents with following ECG in the monitor
intraoperativly
1. What is the diagnosis ?
2. Name two ECG findings that lead to your diagnosis.
3. What is the further line of management?
ECG 6
13.
ECG - 6
1.Supraventricular tachycardia
2. Absent P wave, Narrow QRS, Rate more than 150
3. First step:vagal maneuver
4. Second step:Adenosine 6mg , second dose 12 mg
5. Beta blocker can be given
14.
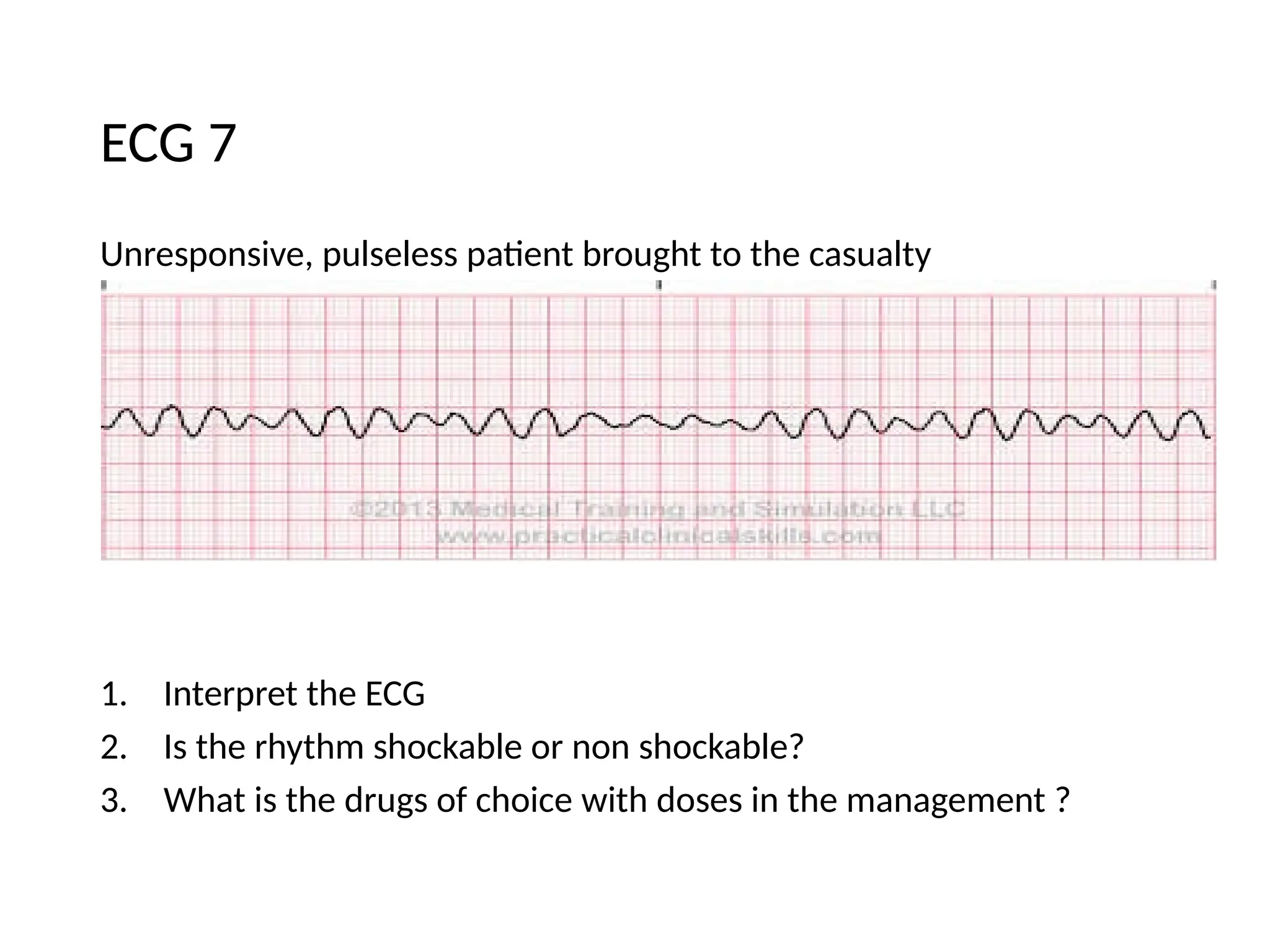
Unresponsive, pulseless patientbrought to the casualty
1. Interpret the ECG
2. Is the rhythm shockable or non shockable?
3. What is the drugs of choice with doses in the management ?
ECG 7
15.
ECG 7
• Ventricularfibrillation
• Shockable rhythm
• After 2nd shock administer Epinephrine 1 mg ,
• After 3rd shock Amiodarone 300mg first dose /Lignocaine 1-
1.5mg/kg
• After 5th shock 150mg 2nd
dose
16.
• Interpret theECG below and answer the following questions
1. What is the rate?
2. What is the diagnosis ?
3. Name one findings to come to the diagnosis.
ECG 8
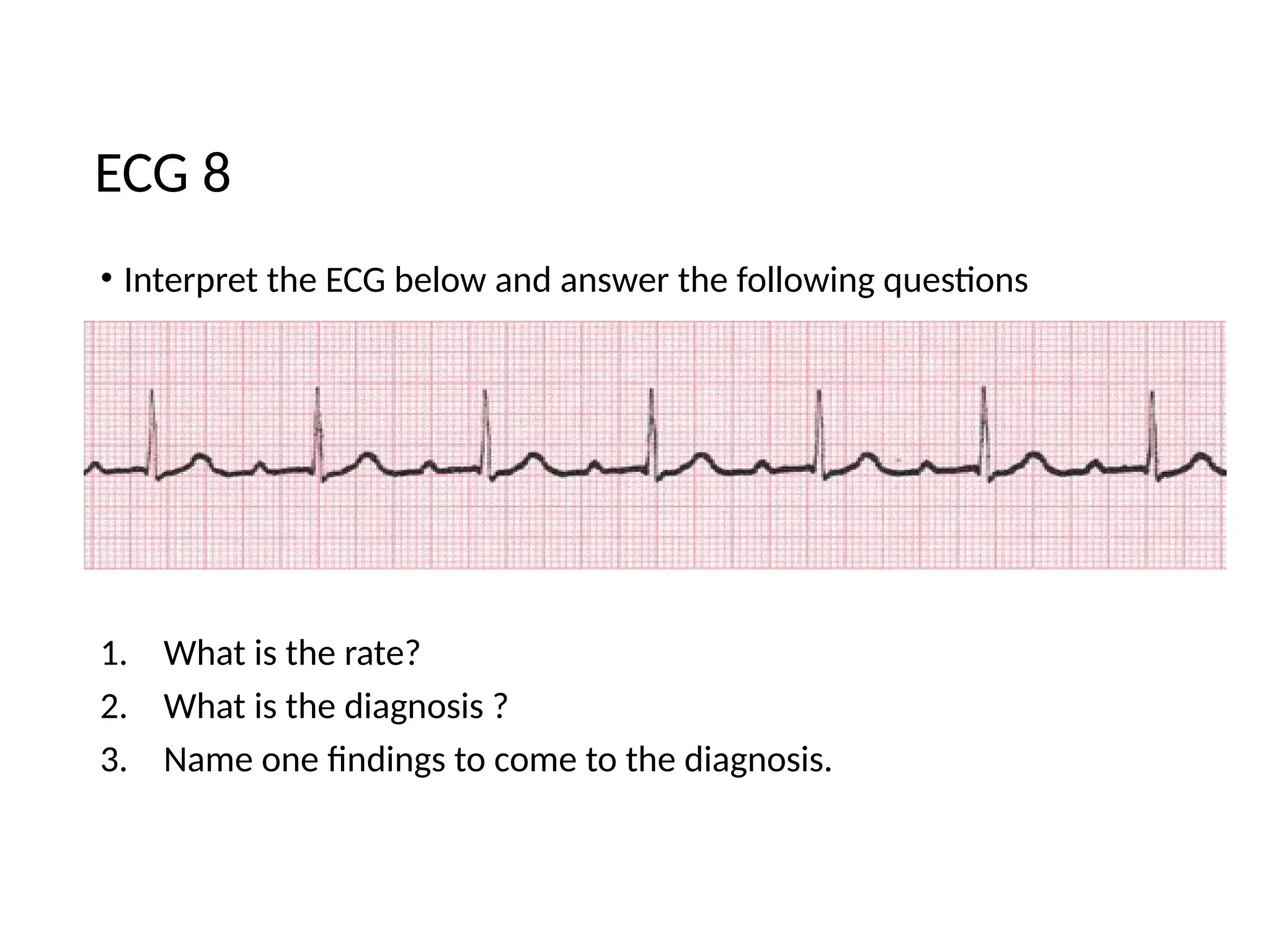
• Interpret theECG below and answer the following questions
1. What is the rate?
2. What is the diagnosis ?
3. Name two findings to come to the diagnosis.
ECG - 9
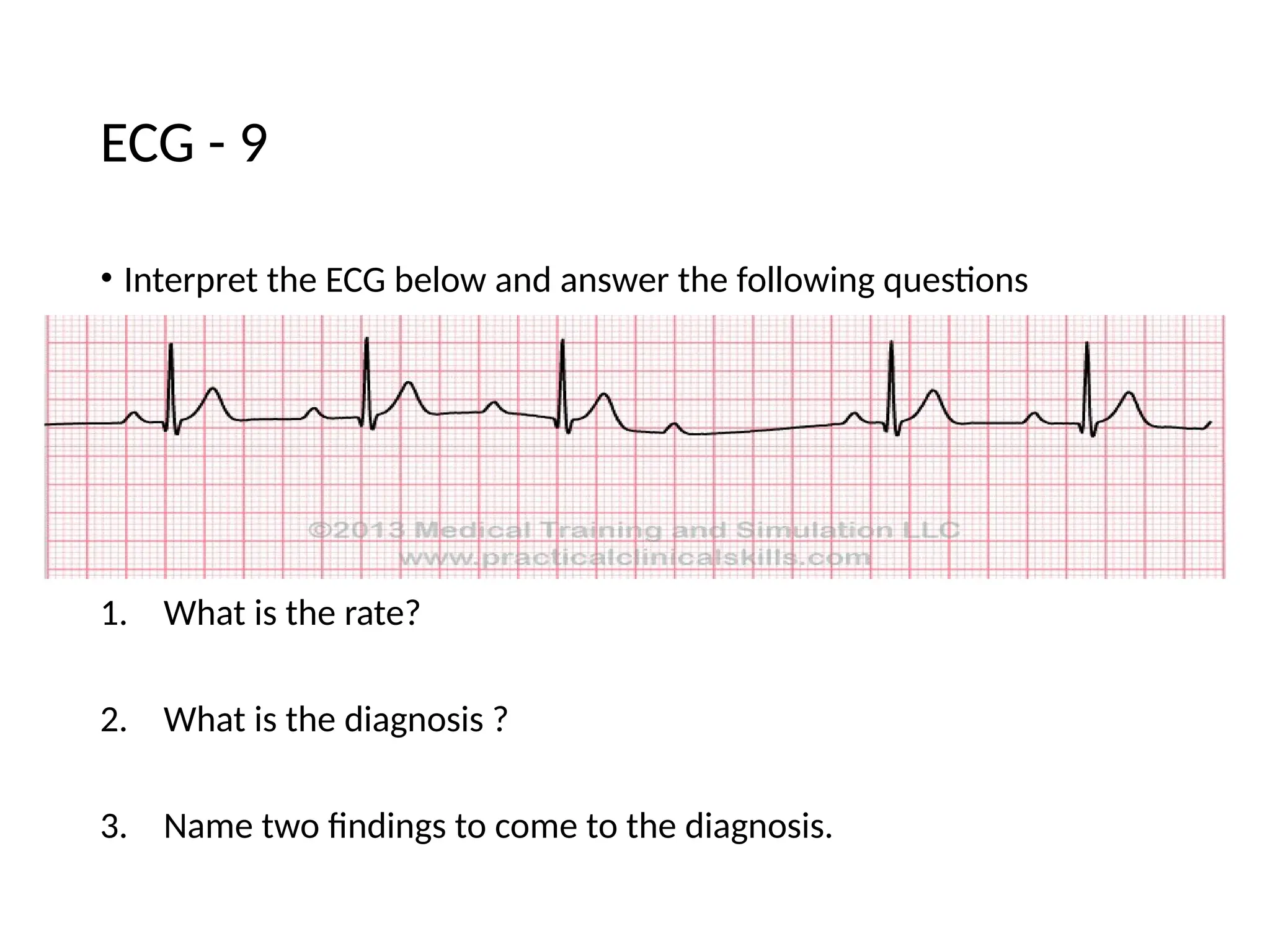
• Interpret theECG below and answer the following questions
1. What is the rate?
2. What is the diagnosis ?
3. Name two findings to come to the diagnosis.
ECG 10
21.
ECG 10
1. 60/min
2.2nd
degree heart block , Mobitz type II
3. Bradycardia , PR interval is constant, irregular RR interval ,2:1
conduction
22.
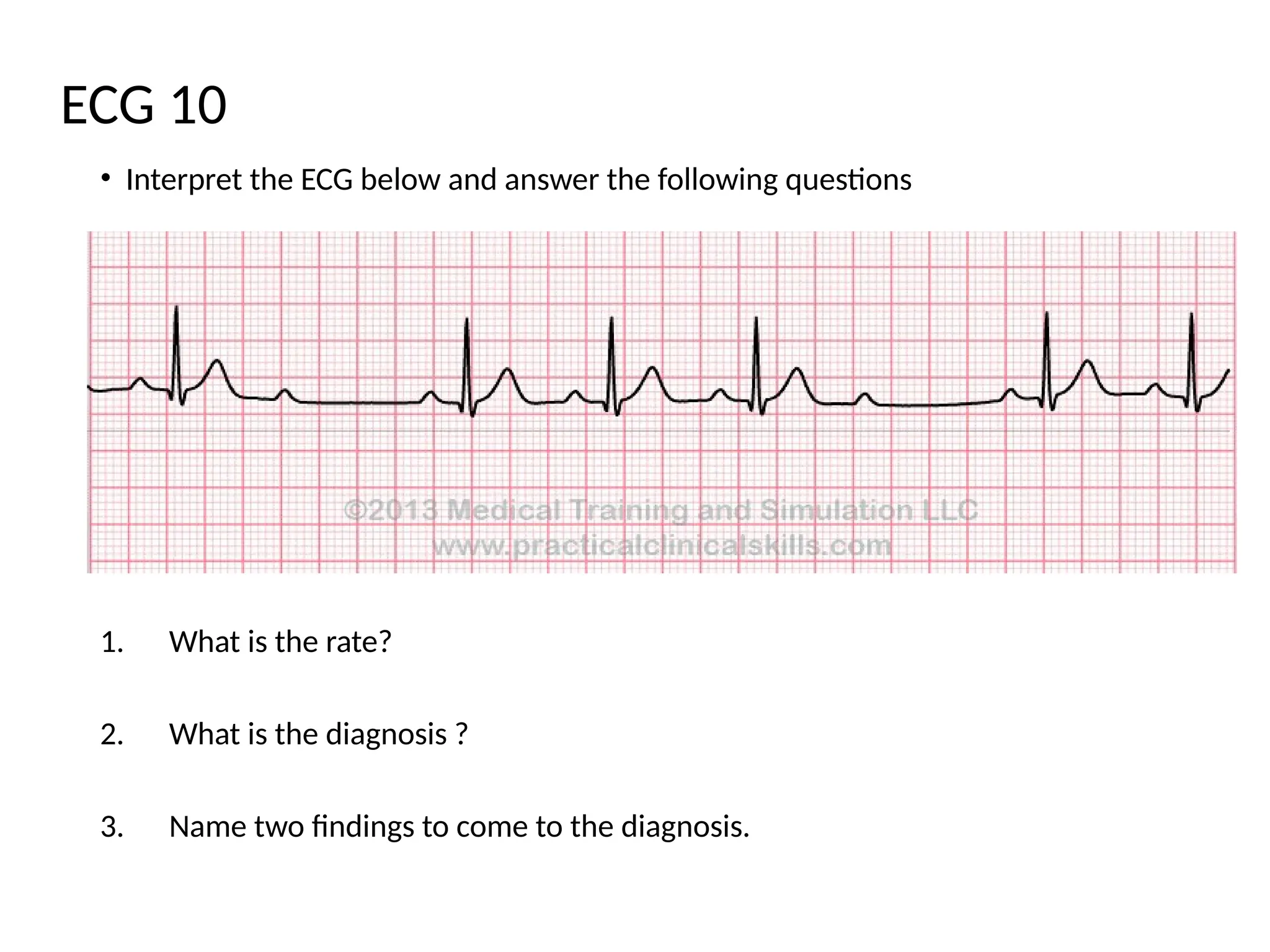
Interpret the ECGbelow and answer the following questions
1. What is the rate?
2. Rhythm - regular/irregular?
3. Calculate PR interval ?
4. What is the diagnosis ?
ECG - 11
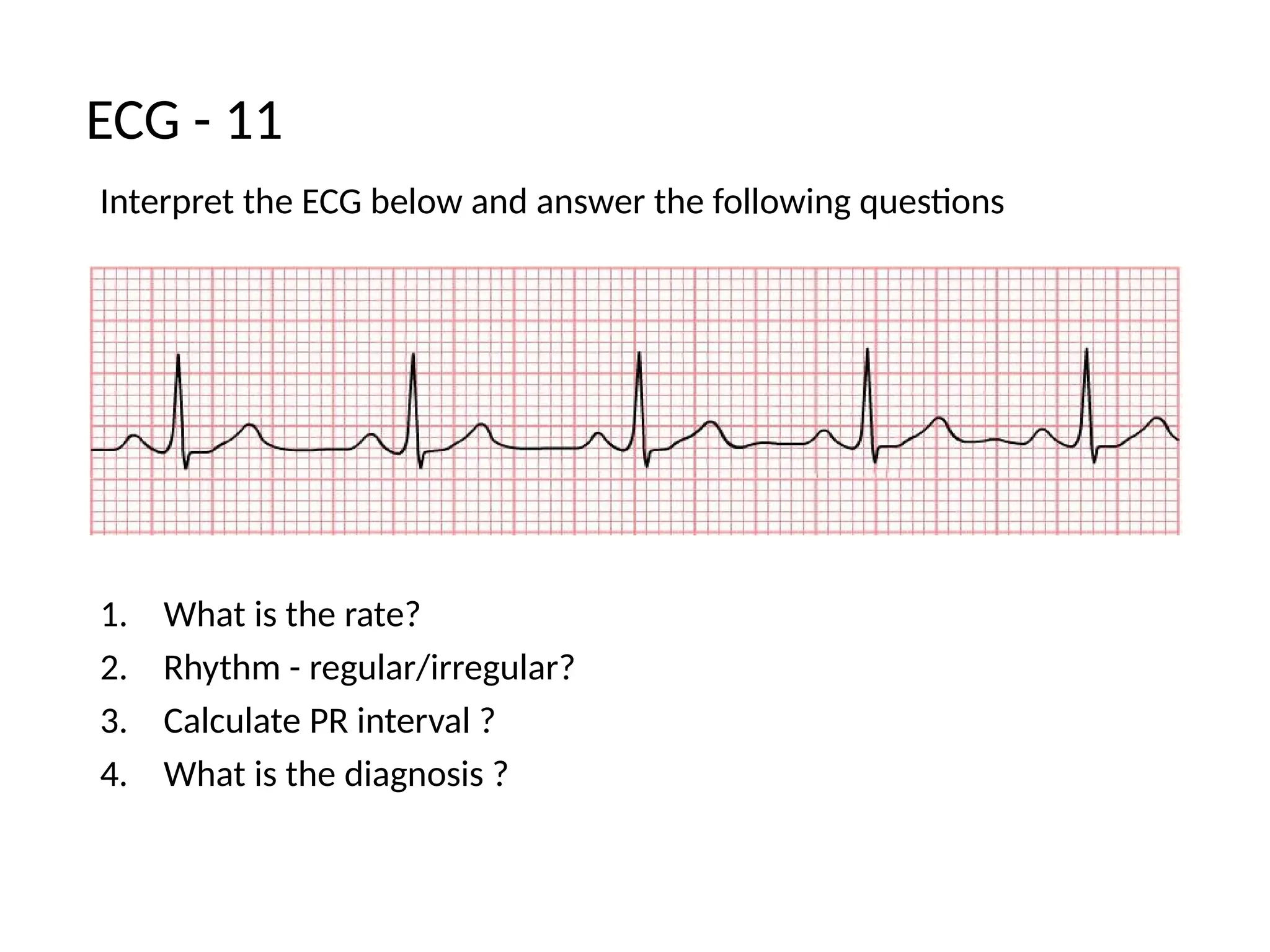
Interpret the ECGbelow and answer the following questions
1. What is the rate?
2. Name two findings to come to the diagnosis.
3. What is the diagnosis ?
ECG - 12
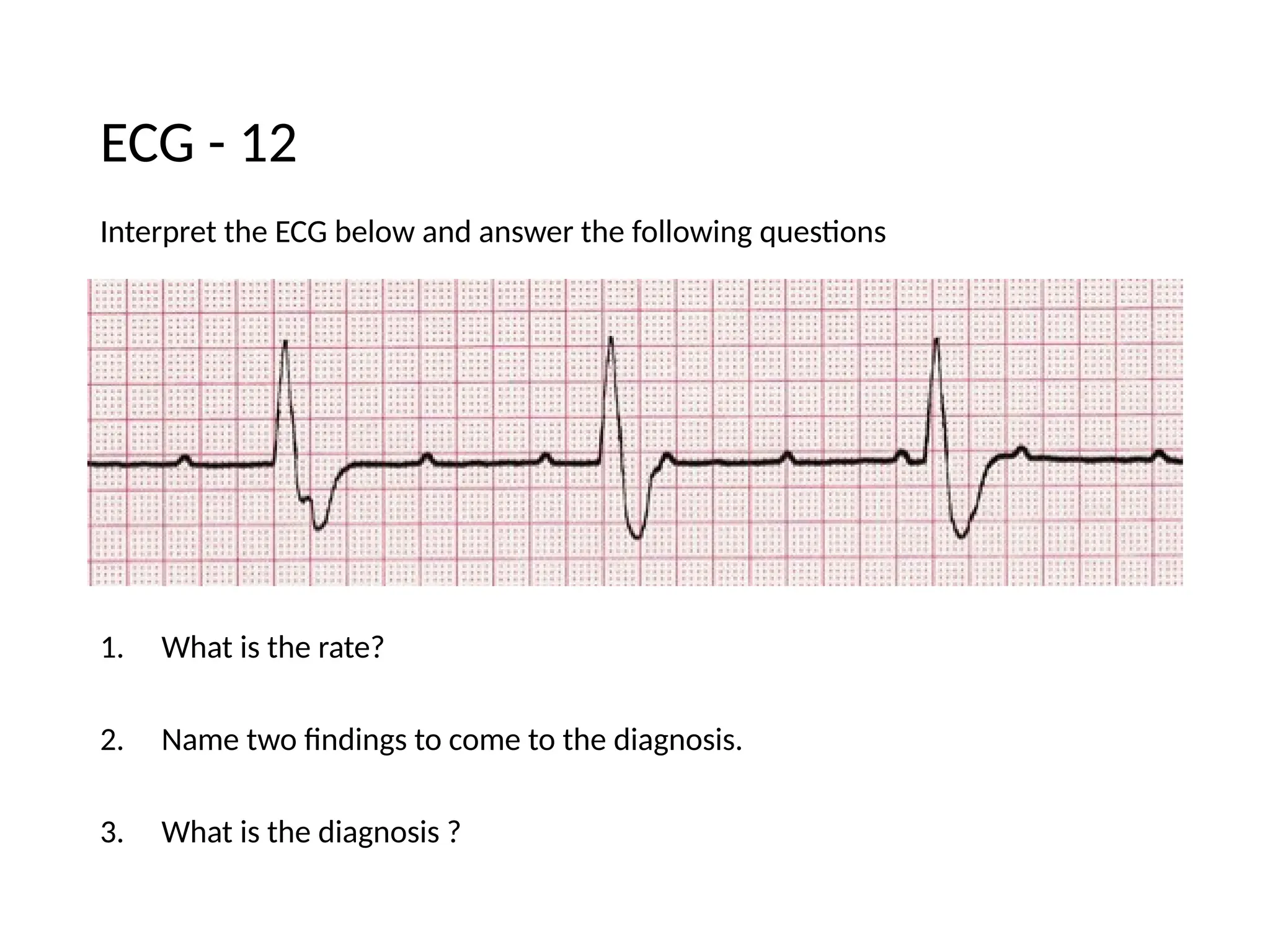
• Interpret theECG below and answer the following questions
1. What is the rate? (1 mark)
2. Comment on P wave characteristics?
3. What is the interpretation ?
4. Which heart chamber enlargement leads to this characteristic?
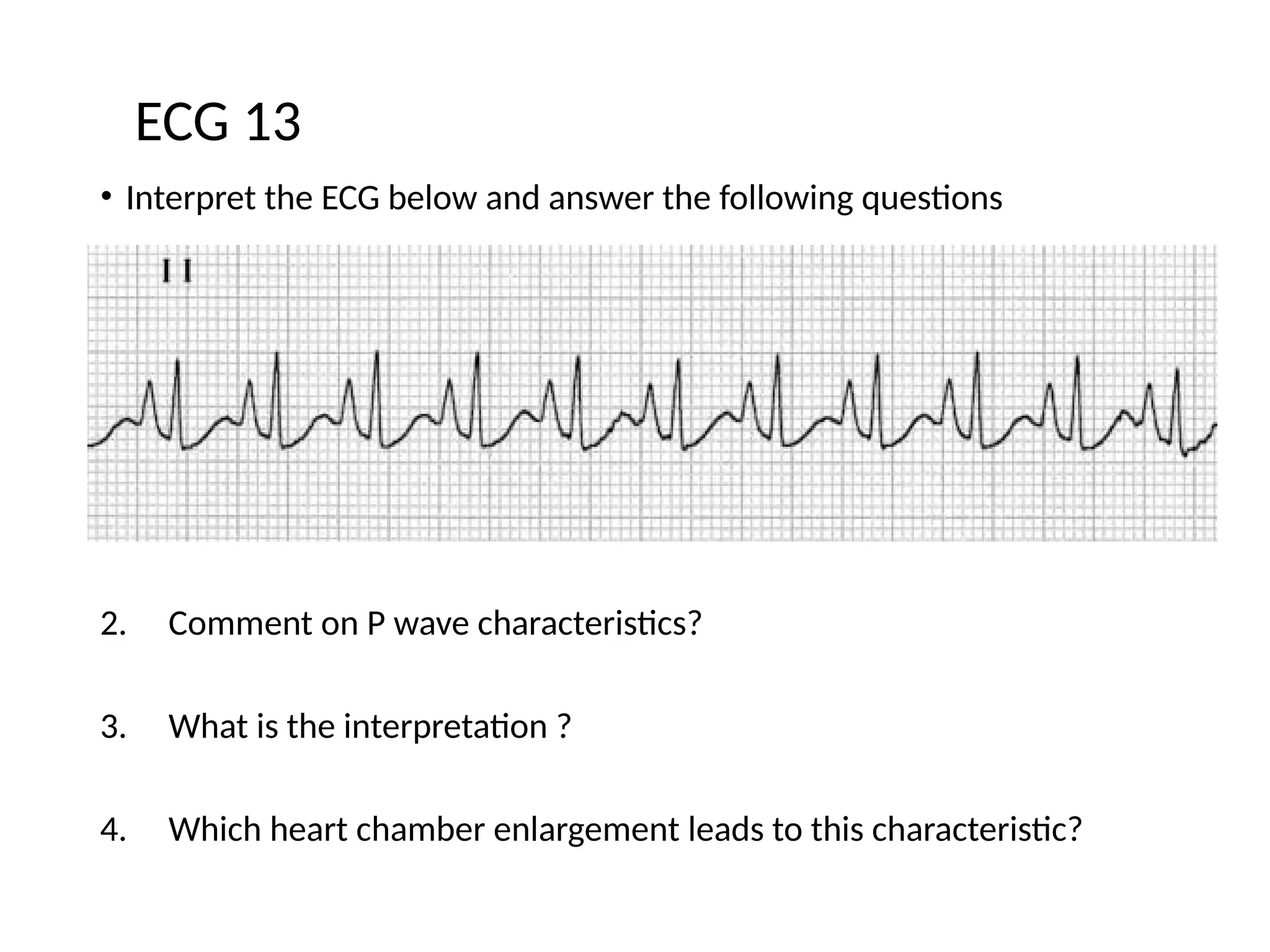
ECG 13
27.
ECG - 13
•150/min
• Tall and peaked P wave
• P Pulmonale
• Right atrial
28.
• Interpret theECG below and answer the following questions
1. What is the rate?
2. Comment on P wave characteristics?
3. What is the interpretation ?
4. Which heart chamber enlargement leads to this characteristic?
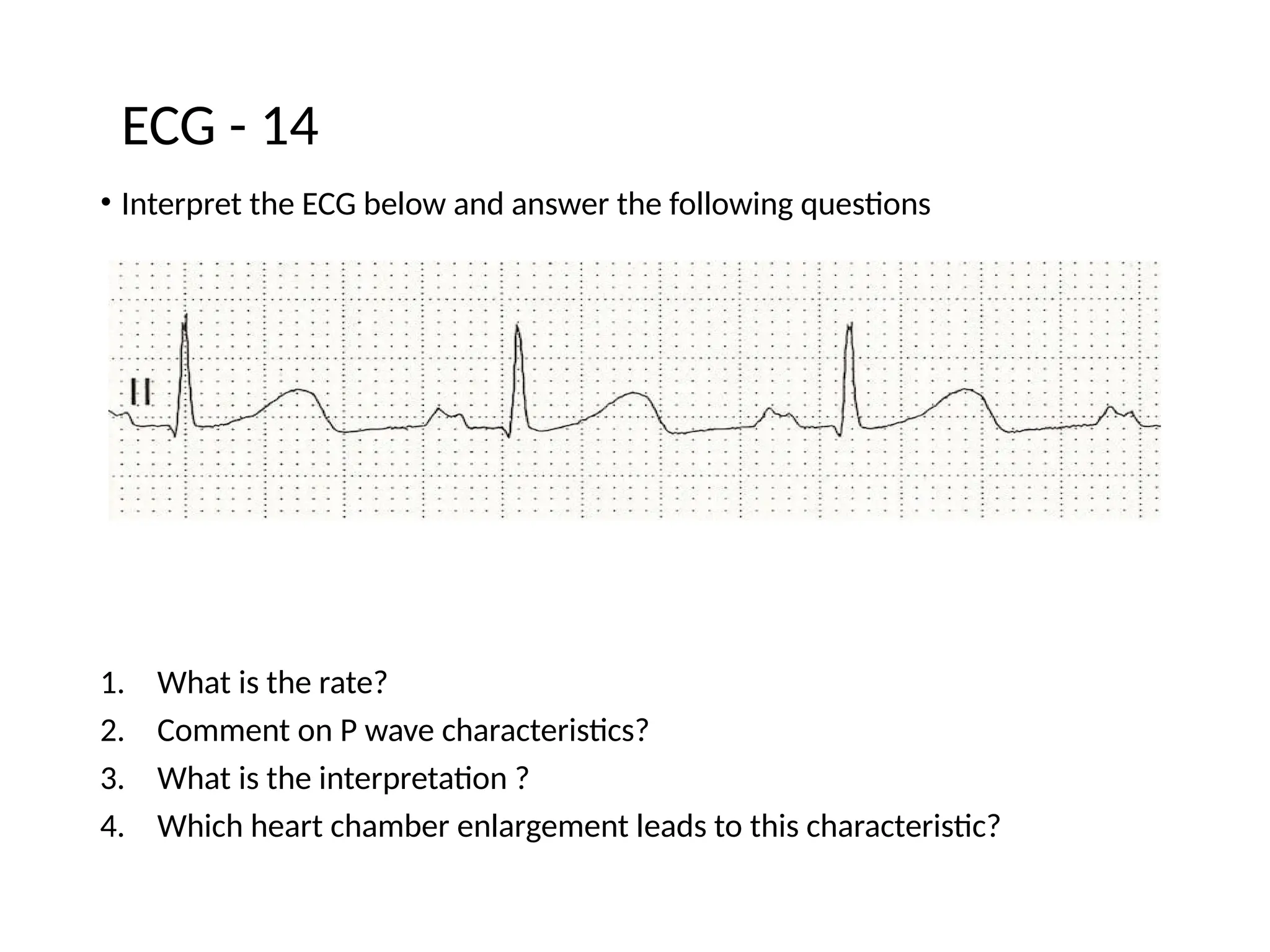
ECG - 14
29.
ECG - 14
1.75/min
2. Broad , double peaked P wave
3. P Mitrale
4. Left Atrium
30.
ECG - 15
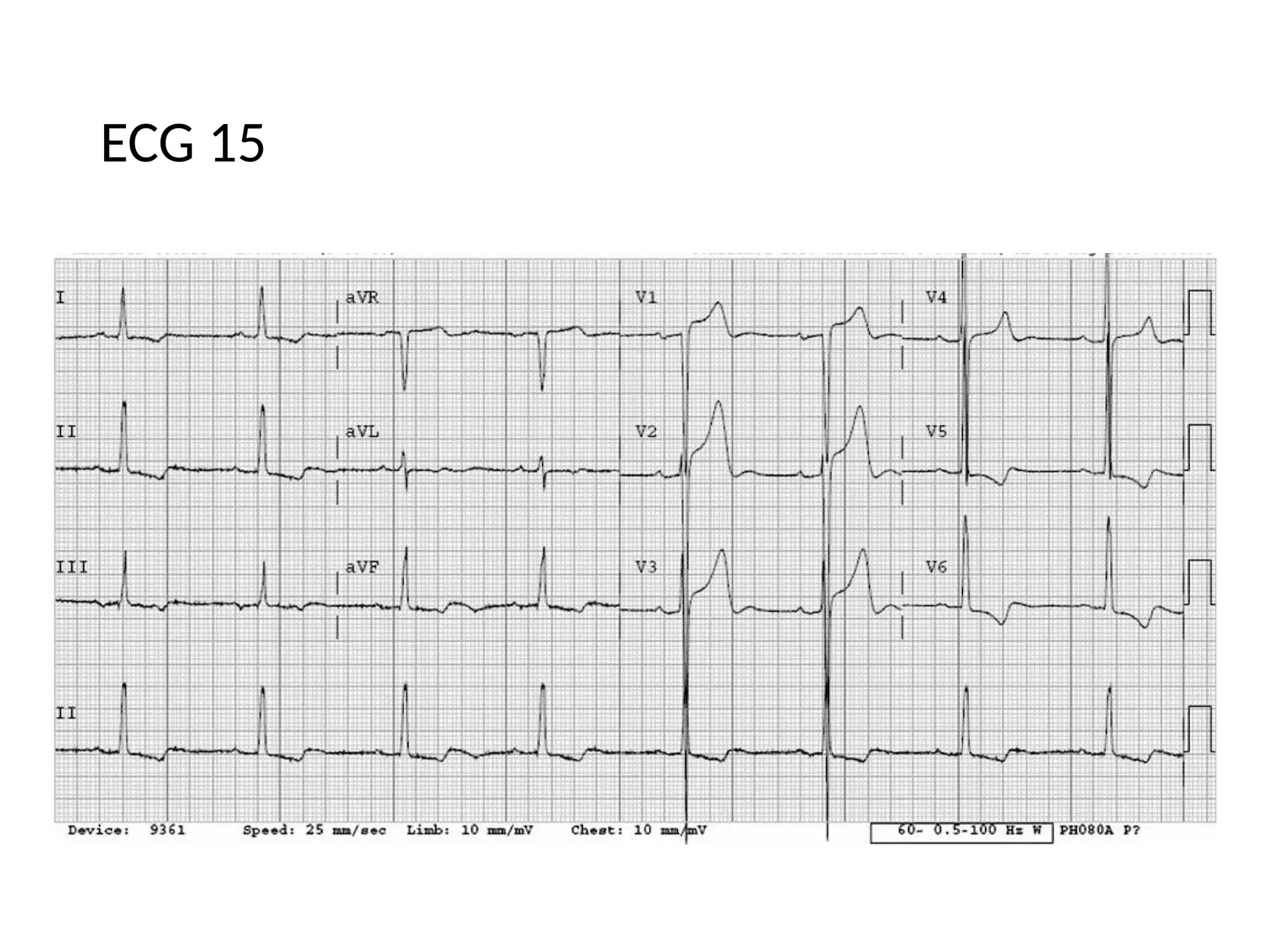
•Interpret the ECG below and answer the following questions
1. What is the rate?
2. Rhythm regular/irregular?
3. What is the diagnosis ?
4. Name the ECG finding that lead to your diagnosis.
ECG 15
1. 50per minute
2. Regular
3. Left ventricular Hypertrophy with strain
4. Rwave in V5 and V6 greater 25 mm, Rwave in V5 and V6 +S wave
in V1V2 greater than 35
33.
ECG - 16
•Interpret the ECG below and answer the following questions
1. What is the rate?
2. Rhythm regular/irregular?
3. What is the diagnosis ?
4. Name the ECG finding that lead to your diagnosis.
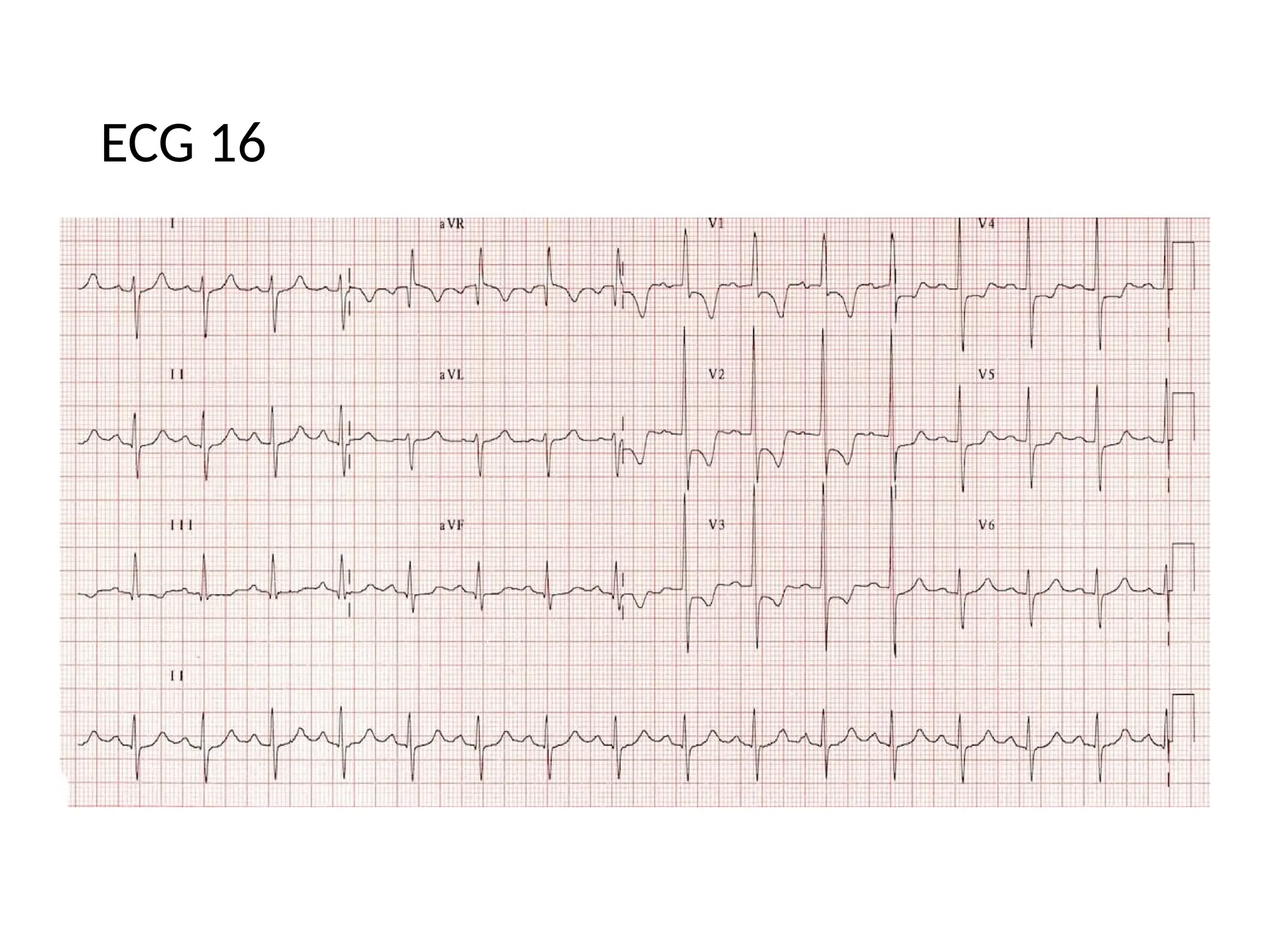
ECG - 16
1.100 per minute
2. Regular
3. Right ventricular hypertrophy
4. Dominant R wave in V1 (> 7mm tall or R/S ratio > 1).Dominant
S wave in V5 or V6 (> 7mm deep or R/S ratio < 1).
36.
ECG 17
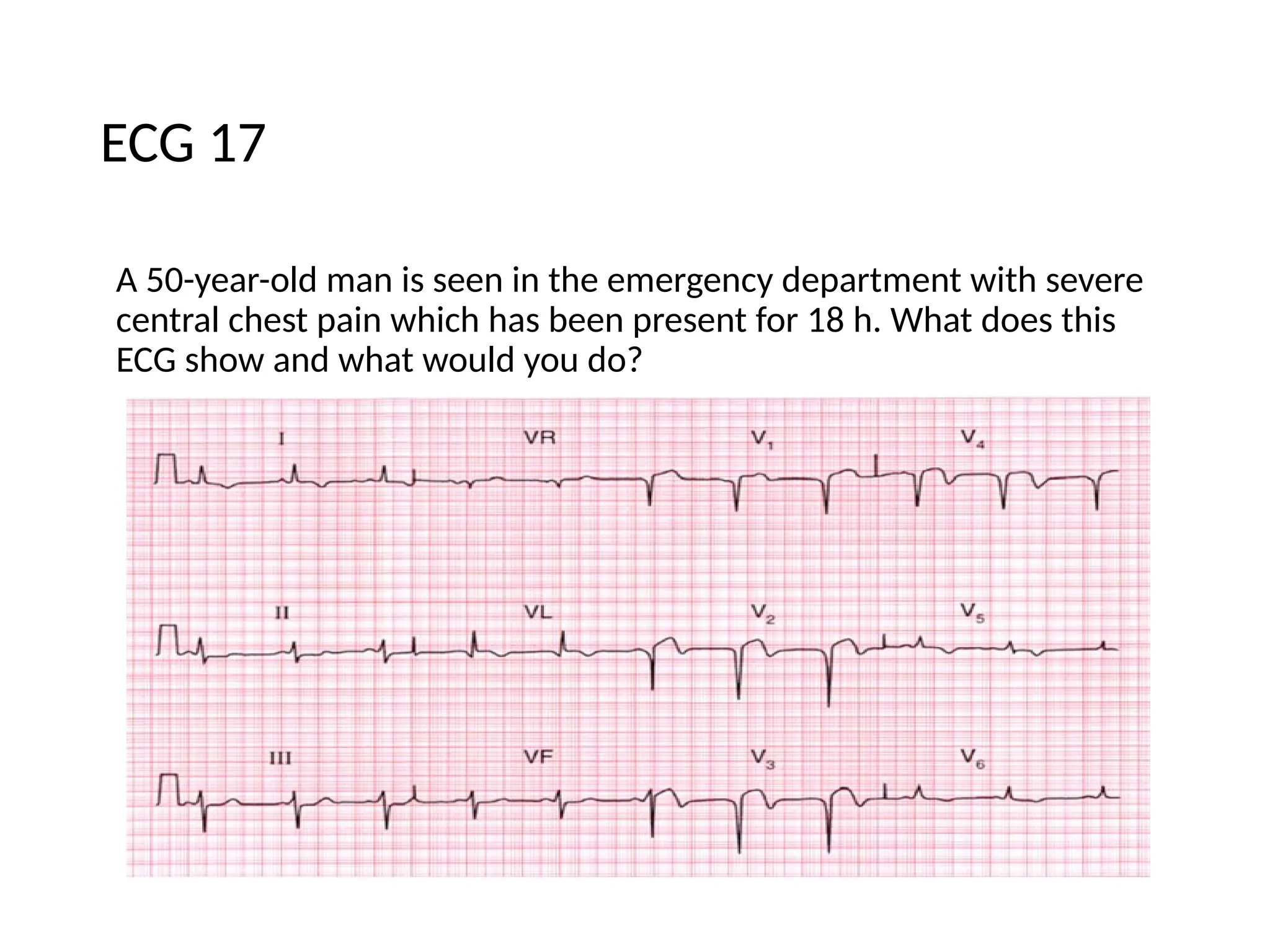
A 50-year-oldman is seen in the emergency department with severe
central chest pain which has been present for 18 h. What does this
ECG show and what would you do?
37.
ECG 17
• TheECG shows:
• Sinus rhythm
• Normal axis
• Q waves in leads V2-V4
• Raised ST segments in leads V2-V4
• Inverted T waves in leads I, VL, V2-V6
Clinical interpretation
This is a classic acute anterior myocardial infarction.
ECG 18
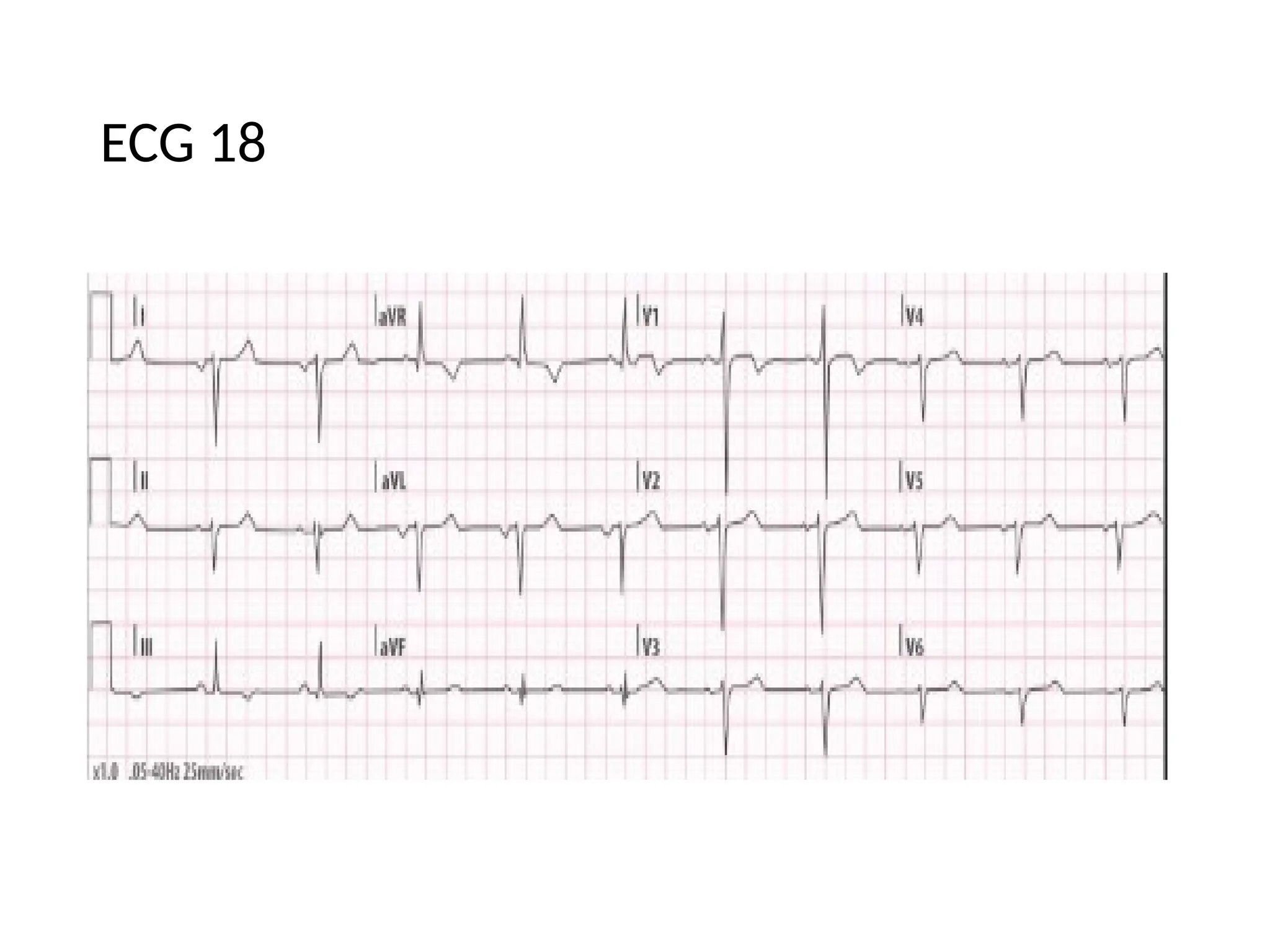
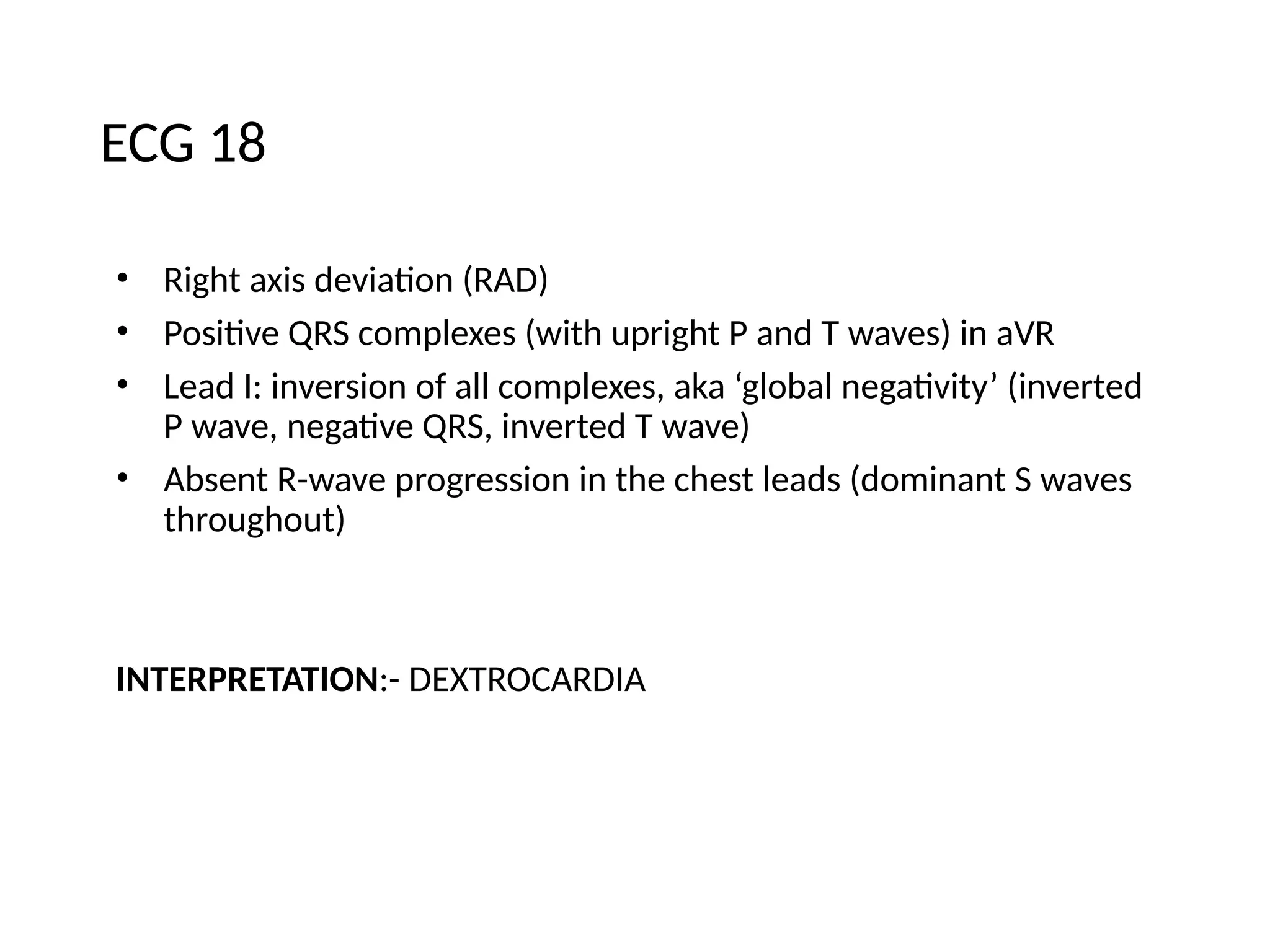
• Rightaxis deviation (RAD)
• Positive QRS complexes (with upright P and T waves) in aVR
• Lead I: inversion of all complexes, aka ‘global negativity’ (inverted
P wave, negative QRS, inverted T wave)
• Absent R-wave progression in the chest leads (dominant S waves
throughout)
INTERPRETATION:- DEXTROCARDIA