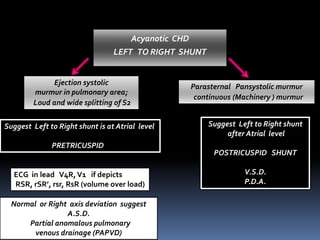
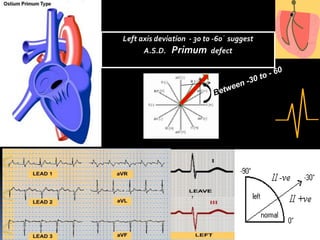
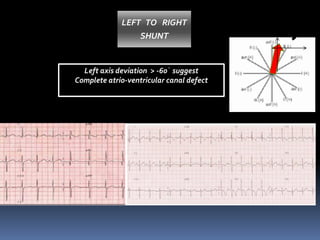
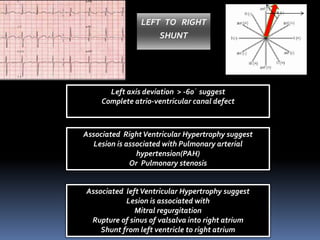
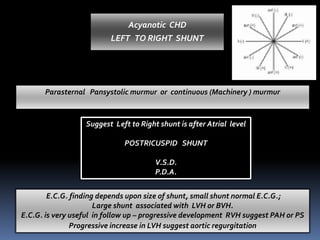
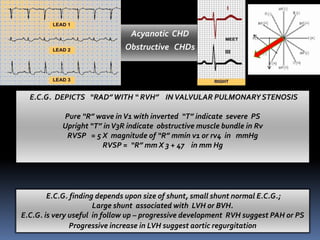
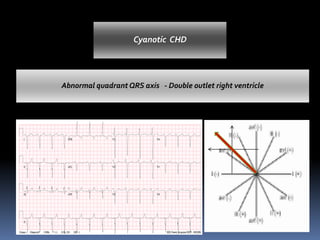
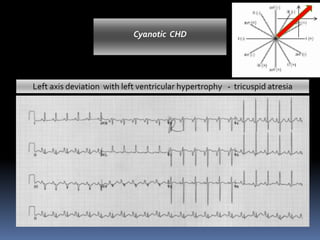
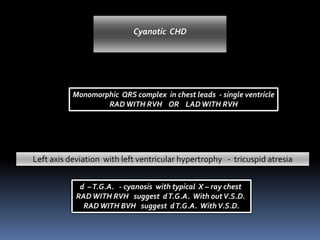
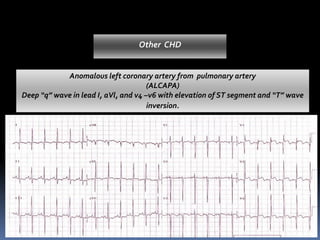
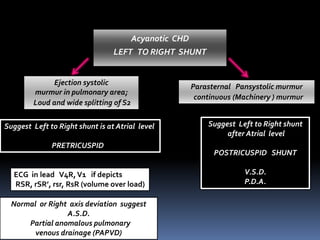
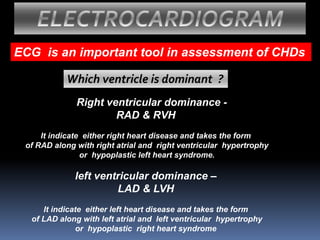
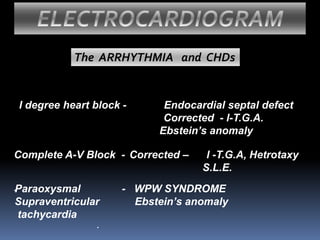
ECG can help diagnose congenital heart defects (CHDs) by reflecting their structural and hemodynamic changes. Specific ECG patterns can indicate the type and location of left-to-right shunts in acyanotic CHDs, such as an RSR' pattern suggesting a pre-tricuspid shunt. ECG findings of right or left ventricular hypertrophy and abnormal axes can also provide clues about underlying CHDs like transposition of the great arteries or tricuspid atresia. Analyzing P waves, QRS complexes, and other ECG components can further help identify conditions like Ebstein's anomaly, anomalous coronary arteries, or corrected transposition of the great arteries.







































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)










