









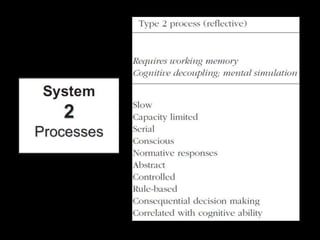

















































This document discusses clinical reasoning in physical therapy. It defines clinical reasoning as the thinking that underpins clinical practice, involving cognitive, intuitive, and mental operations that lead to decision making. It discusses different types of clinical reasoning such as intuitive, reflective, inductive, deductive, and Bayesian reasoning. It also discusses the dual process theory of reasoning and the continuum between intuitive and reflective reasoning. The document explores how clinical reasoning is developed through experience, education, and different learning activities. It emphasizes that clinical reasoning involves associating related data from different categories to build clinical patterns.





























































