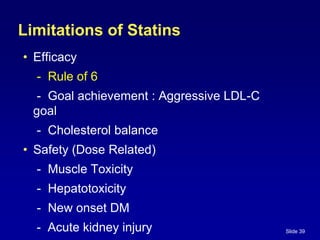
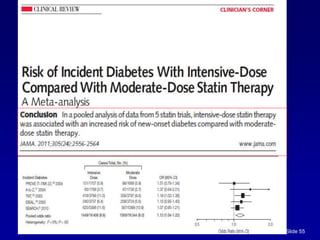
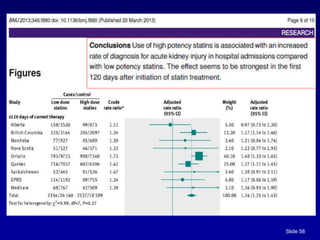
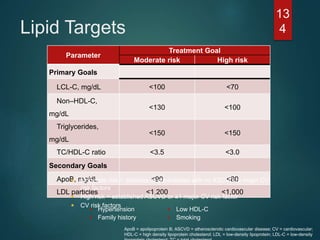
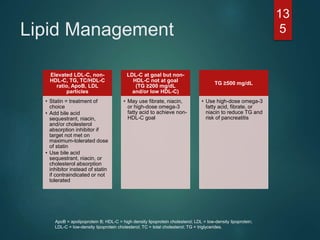
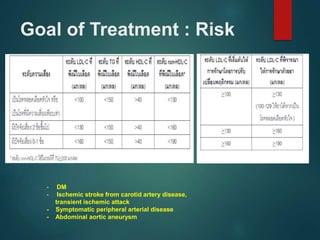
This document discusses dyslipidemia and its management. It begins by outlining how elevated cholesterol is a risk factor for cardiovascular disease. It then discusses screening guidelines and treatment goals for LDL cholesterol levels. The rest of the document covers lifestyle and pharmacological treatment options for dyslipidemia, with a focus on statin drugs and their limitations. It provides details on statin efficacy, safety concerns, and the additional benefits of combining statins with other drugs like ezetimibe.
![ First diagnosis of DM,
And/or at age 40 years
And periodically (e.g., every 1–2 years)
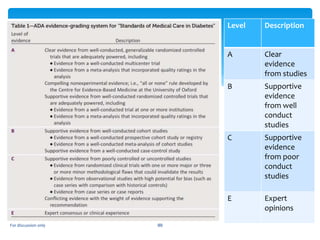
Level E [ expert opinion ]
Screening lipid profile](https://image.slidesharecdn.com/dyslipidemiaezetrol-230224014416-8e786685/85/dyslipidemia-ezetrol-pptx-17-320.jpg)
















![PHARMACOTHERAPY POINTERS FOR ATHEROSCLEROSIS [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforatherosclerosismalaysiancpgs-230519014441-00a85dfd-thumbnail.jpg?width=640&height=640&fit=bounds)




































