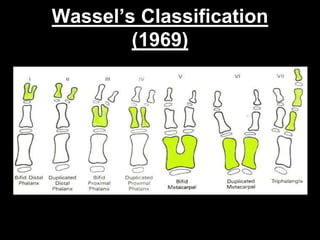
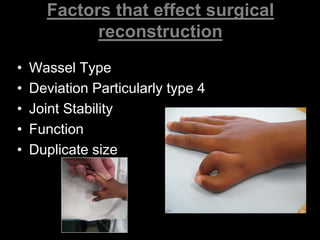
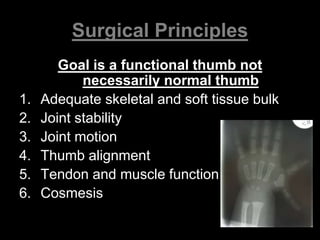
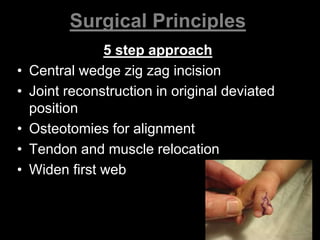
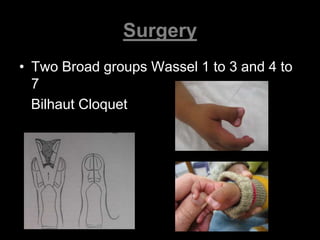
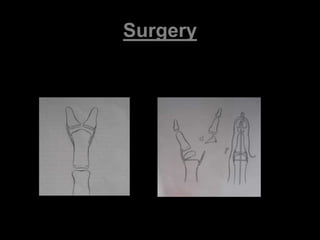
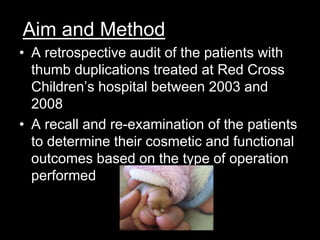
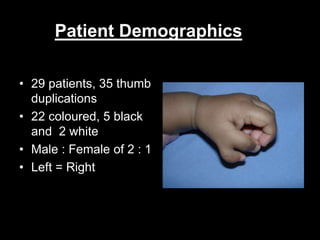
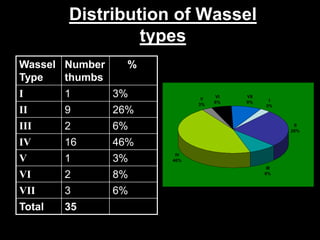
This document discusses the surgical management of duplicated thumbs. It begins by classifying duplicated thumbs and noting their prevalence. Type IV duplications, which involve joint deviation, are the most common. The document outlines factors that affect reconstruction surgery like the Wassel classification type and degree of deviation. The surgical principles aim for a functional thumb with adequate structure, stability, motion, alignment, and tendon function. The document then describes the retrospective study of 29 patients at Red Cross Children's Hospital between 2003-2008 who underwent thumb duplication surgery. It analyzes outcomes based on Wassel type and surgery performed, noting that stability at the thumb joints is essential for function and excision with ligament reconstruction yields good functional and cosmetic results.