
Downloaded 45 times
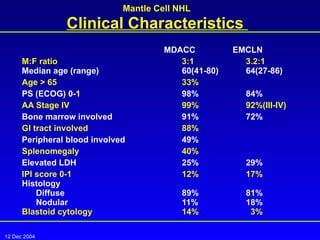
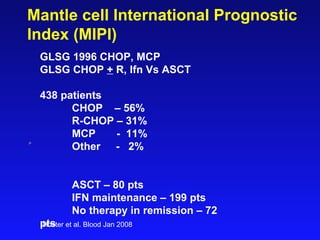
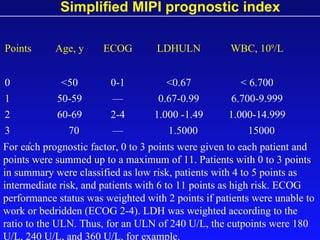
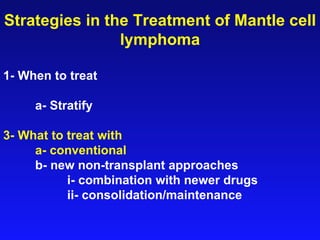

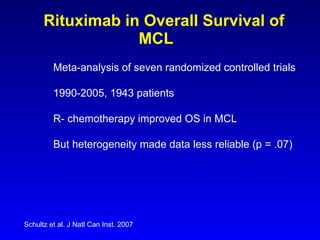
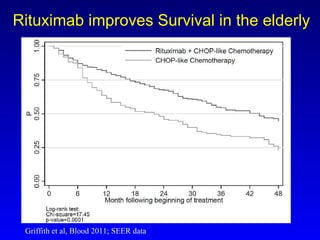
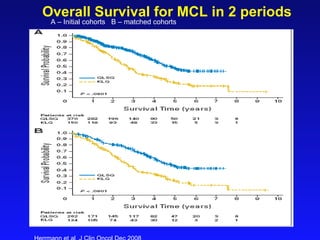
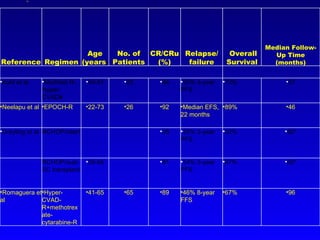
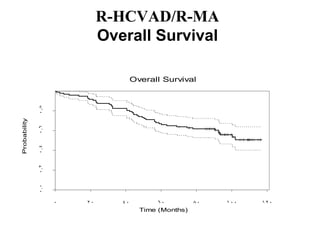
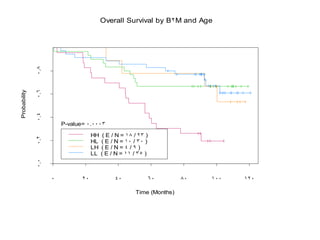
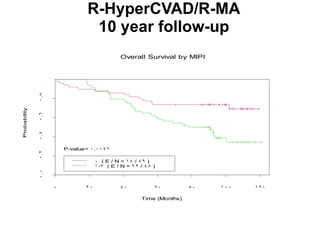
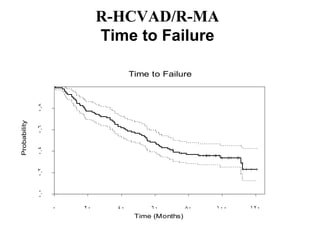
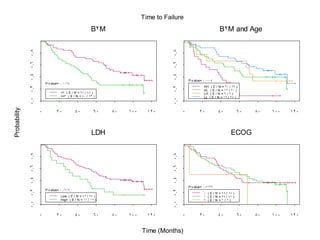
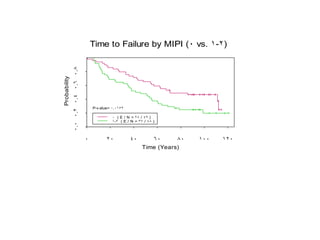
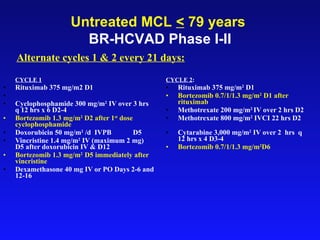
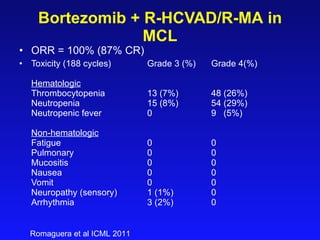
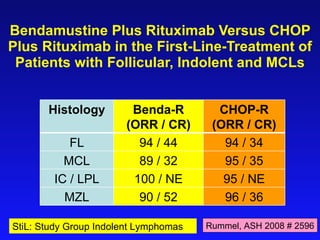
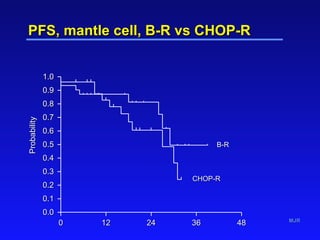
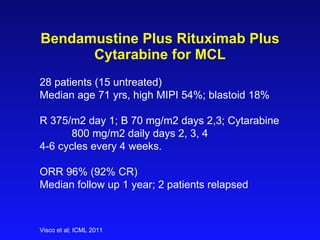

This document summarizes strategies for treating mantle cell lymphoma (MCL), including: - When to treat: stratifying based on prognostic factors like the Mantle Cell International Prognostic Index (MIPI) - What to treat with: conventional chemotherapy like R-CHOP plus newer drugs like bortezomib; more intensive regimens including Hyper-CVAD have shown improved survival - Rituximab improves outcomes and its addition to chemotherapy is recommended - Bendamustine plus rituximab has efficacy comparable to R-CHOP for MCL























































































