Welcome!
Please be seatedquietly and begin Quiz 3 in Canvas.
It is open book. You have 1 hour to answer 30 multiple choice questions.
You may take a break when finished and return to start class in keeping
with the agenda.
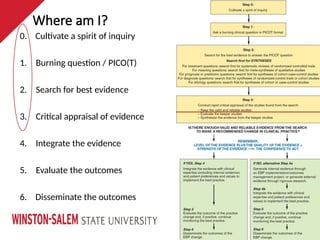
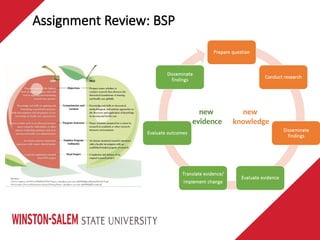
0. Cultivate aspirit of inquiry
1. Burning question / PICO(T)
2. Search for best evidence
3. Critical appraisal of evidence
4. Integrate the evidence
5. Evaluate the outcomes
6. Disseminate the outcomes
Where am I?
Assignment Review: BSP
•Clinical problem in the population
• Current knowledge
• Disparity/inequity
• Supporting data/evidence
• Local/practice site problem
• Relevant quality indicator
• Literature review purpose
• Clinical question (PICOT)
• Gaps in literature
• Search strategy & results
13.
Assignment Review: BSP
•Clinical problem in the population
• Current knowledge
• Disparity/inequity
• Supporting data/evidence
• Local/practice site problem
• Relevant quality indicator
• Literature review purpose
• Clinical question (PICOT)
• Gaps in literature
• Search strategy & results
14.
Assignment Review: BSP
•Clinical problem in the population
• Current knowledge
• Disparity/inequity
• Supporting data/evidence
• Local/practice site problem
• Relevant quality indicator
• Literature review purpose
• Clinical question (PICOT)
• Gaps in literature
• Search strategy & results
15.
Assignment Review: BSP
•Clinical problem in the population
• Current knowledge
• Disparity/inequity
• Supporting data/evidence
• Local/practice site problem
• Relevant quality indicator
• Literature review purpose
• Clinical question (PICOT)
• Gaps in literature
• Search strategy & results
Assignment Review: BSP
•Clinical problem in the population
• Current knowledge
• Disparity/inequity
• Supporting data/evidence
• Local/practice site problem
• Relevant quality indicator
• Literature review purpose
• Clinical question (PICOT)
• Gaps in literature
• Search strategy & results
19.
The GAP
• GAP
•Something that remains to be done or learned in an area of study
• knowledge/evidence of scientific literature
• missing pieces
• not yet explored or underexplored
• Project must address a gap in order to make a contribution to nursing science
http://sites.middlebury.edu/middsciwriting/overview/organization/gap-statements/
Assignment Review: BSP
20.
Identify the GAP
•Succinctly identify the gap(s) project will attempt to address
• What has/has not been learned from the review of the literature?
• What did the authors find/discuss and what did they suggest as future areas of study?
• Ask critical questions as compare/contrast studies re population, setting, conditions, variables,
methods, analysis, measurement or outcomes.
• Problem
• what variances and similarities do see between clinical scenario and literature?
• epidemiology , processes, structures/resources, etc.
• Intervention
• is there a paucity of evidence in a particular setting or with the population of interest?
http://sites.middlebury.edu/middsciwriting/overview/organization/gap-statements/
Assignment Review: BSP
21.
Identify the GAP
•What is unique or innovative about your project?
• Signal phrases
• has/have not been studied/reported/elucidated…
• is required/needed…
• the key question is/remains…
• it is important to address…
http://sites.middlebury.edu/middsciwriting/overview/organization/gap-statements/
Assignment Review: BSP
22.
Fill the GAP
•Create summary statement about how project will attempt to fill the gap
• State the project purpose
• The purpose of this project is to…
• Indicate the gaps the project will fill
• This project will address gaps in…
Assignment Review: BSP
23.
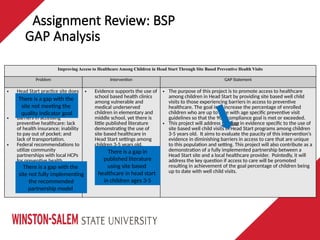
GAP Analysis
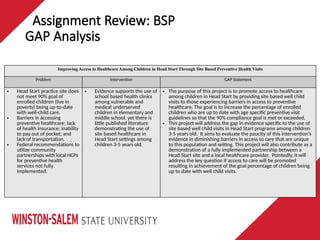
Improving Accessto Healthcare Among Children in Head Start Through Site Based Preventive Health Visits
Problem Intervention GAP Statement
• Head Start practice site does
not meet 90% goal of
enrolled children (live in
poverty) being up-to-date
with well-child care.
• Barriers in accessing
preventive healthcare: lack
of health insurance; inability
to pay out of pocket; and
lack of transportation.
• Federal recommendations to
utilize community
partnerships with local HCPs
for preventive health
services not fully
implemented.
• Evidence supports the use of
school based health clinics
among vulnerable and
medical underserved
children in elementary and
middle school, yet there is
little published literature
demonstrating the use of
site based healthcare in
Head Start settings among
children 3-5 years old.
• The purpose of this project is to promote access to healthcare
among children in Head Start by providing site based well child
visits to those experiencing barriers in access to preventive
healthcare. The goal is to increase the percentage of enrolled
children who are up to date with age specific preventive visit
guidelines so that the 90% compliance goal is met or exceeded.
• This project will address the gap in evidence specific to the use of
site based well child visits in Head Start programs among children
3-5 years old. It aims to evaluate the paucity of this intervention’s
evidence in diminishing barriers in access to care that are unique
to this population and setting. This project will also contribute as a
demonstration of a fully implemented partnership between a
Head Start site and a local healthcare provider. Pointedly, it will
address the key question if access to care will be promoted
resulting in achievement of the goal percentage of children being
up to date with well child visits.
Assignment Review: BSP
24.
GAP Analysis
Improving Accessto Healthcare Among Children in Head Start Through Site Based Preventive Health Visits
Problem Intervention GAP Statement
• Head Start practice site does
not meet 90% goal of
enrolled children (live in
poverty) being up-to-date
with well-child care.
• Barriers in accessing
preventive healthcare: lack
of health insurance; inability
to pay out of pocket; and
lack of transportation.
• Federal recommendations to
utilize community
partnerships with local HCPs
for preventive health
services not fully
implemented.
• Evidence supports the use of
school based health clinics
among vulnerable and
medical underserved
children in elementary and
middle school, yet there is
little published literature
demonstrating the use of
site based healthcare in
Head Start settings among
children 3-5 years old.
• The purpose of this project is to promote access to healthcare
among children in Head Start by providing site based well child
visits to those experiencing barriers in access to preventive
healthcare. The goal is to increase the percentage of enrolled
children who are up to date with age specific preventive visit
guidelines so that the 90% compliance goal is met or exceeded.
• This project will address the gap in evidence specific to the use of
site based well child visits in Head Start programs among children
3-5 years old. It aims to evaluate the paucity of this intervention’s
evidence in diminishing barriers in access to care that are unique
to this population and setting. This project will also contribute as a
demonstration of a fully implemented partnership between a
Head Start site and a local healthcare provider. Pointedly, it will
address the key question if access to care will be promoted
resulting in achievement of the goal percentage of children being
up to date with well child visits.
There is a gap with the
site not meeting the
quality indicator goal
There is a gap with the
site not fully implementing
the recommended
partnership model
There is a gap in
published literature
using site based
healthcare in head start
in children ages 3-5
Assignment Review: BSP
Assignment Review: BSP
•Clinical problem in the population
• Current knowledge
• Disparity/inequity
• Supporting data/evidence
• Local/practice site problem
• Relevant quality indicator
• Literature review purpose
• Clinical question (PICOT)
• Gaps in literature
• Search strategy & results
27.
Assignment Review: BSP
•Clinical problem in the population
• Current knowledge
• Disparity/inequity
• Supporting data/evidence
• Local/practice site problem
• Relevant quality indicator
• Literature review purpose
• Clinical question (PICOT)
• Gaps in literature
• Search strategy & results
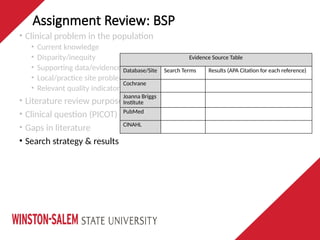
Evidence Source Table
Database/Site Search Terms Results (APA Citation for each reference)
Cochrane
Joanna Briggs
Institute
PubMed
CINAHL
28.
Assignment Review: BSP
•Clinical problem in the population
• Current knowledge
• Disparity/inequity
• Supporting data/evidence
• Local/practice site problem
• Relevant quality indicator
• Literature review purpose
• Clinical question (PICOT)
• Literature review purpose
• Clinical question (PICOT)
• Gaps in literature
• Search strategy & results
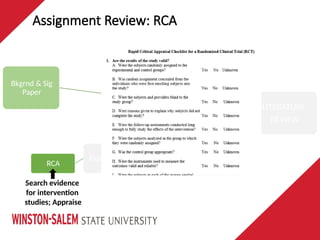
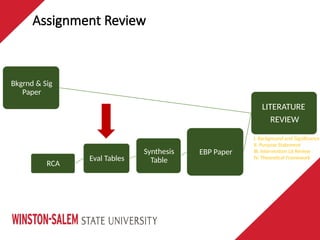
Assignment Review: EvaluationTables
LITERATURE
REVIEW
Bkgrnd & Sig
Paper
EBP Paper
Synthesis
Table
Eval Tables
RCA
ID keeper
intervention studies
& further analyze
31.
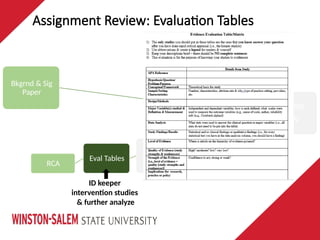
Assignment Review: EvaluationTables
LITERATURE
REVIEW
Bkgrnd & Sig
Paper
EBP Paper
Synthesis
Table
Eval Tables
RCA
ID keeper
intervention studies
& further analyze
32.
Assignment Review
LITERATURE
REVIEW
Bkgrnd &Sig
Paper
EBP Paper
Synthesis
Table
Eval Tables
RCA
I. Background and Significance
II. Purpose Statement
III. Intervention Lit Review
IV. Theoretical Framework
33.
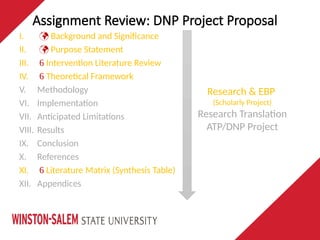
Assignment Review: DNPProject Proposal
I. Background and Significance
II. Purpose Statement
III. Intervention Literature Review
IV. Theoretical Framework
V. Methodology
VI. Implementation
VII. Anticipated Limitations
VIII. Results
IX. Conclusion
X. References
XI. Literature Matrix (Synthesis Table)
XII. Appendices
Research & EBP
(Scholarly Project)
Research Translation
ATP/DNP Project
DNP Essentials &Competency Assessment
DNP degree prepares APNs to meet needs of complex healthcare system by
improving systems of care through research translation that promotes
positive population health outcomes
DNP Essentials are foundational competencies
Essential I: Scientific Underpinnings for Practice
Essential II: Organizational Leadership & Systems Leadership for QI & Systems
Thinking
Essential III: Clinical Scholarship and Analytical Methods for Evidence-Based Practice
Essential IV: Information Systems/Technology and Patient Care Technology for the
Improvement and Transformation of Health Care
Essential V: Health Care Policy for Advocacy in Health Care
Essential VI: Inter-professional Collaboration for Improving Patient and Population
Health Outcomes
Essential VII: Clinical Prevention and Population Health for Improving the Nation’s
Health
Essential VIII: Advanced Nursing Practice
36.
I. Scientific underpinningsfor practice
• strong scientific foundation for practice
• theories to guide nursing practice
III. Clinical scholarship & analytical methods for evidence-based practice
• discovering and integrating new knowledge
• applying knowledge to solve a problem
• translate research into practice, evaluate practice, improve practice and outcomes
VII. Clinical Prevention and Population Health for Improving the Nation’s
Health
• integrate and institutionalize evidence-based clinical prevention and population
health services for populations
• analyze epidemiological, biostatistical, occupational, and environmental data in
the development, implementation, and evaluation of clinical prevention and
population health
DNP Essentials & Competency Assessment
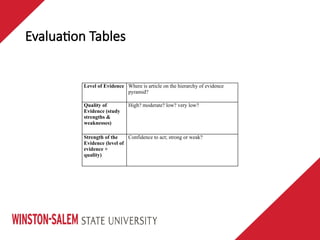
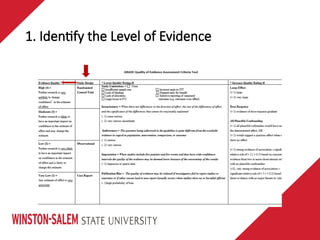
Evaluation Tables
Level ofEvidence Where is article on the hierarchy of evidence
pyramid?
Quality of
Evidence (study
strengths &
weaknesses)
High? moderate? low? very low?
Strength of the
Evidence (level of
evidence +
quality)
Confidence to act; strong or weak?
GRADE
• Grading ofRecommendations, Assessment, Development, and Evaluation
• A systematic method of assessing the quality of studies
• Working Group formed in 2000
• Aim: to develop a common, transparent and sensible system for grading
the quality of evidence and the strength of recommendations
• from evidence to decision
Hockenbury, M (2012). NUR650: Evaluating the quality of evidence, module 3 notes {PowerPoint slides}. Duke University, Durham,
42.
GRADE
Falck-Ytter, Y. &Schunemann (2009). Rating the evidence: Using Grade to develop clinical practice guidelines. {PowerPoint slides}.
Retrieved fromhttps://www.slideshare.net/yashika54/development-of-clinical-practice-guidelines-and-the-grade-approach?qid=858a641c-aede-47ac-8f0d-71099125bc14&v=&b=&from_search=
43.
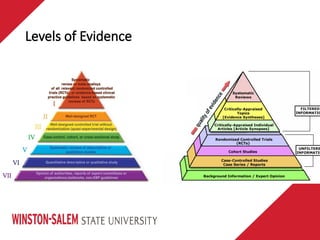
GRADE
• Better researchprovides increased confidence in evidence to support a
particular recommendation
• As level of evidence increases, quality of evidence increases
• RCTs without important limitations provide high quality evidence
• Observational studies without special strengths provide low quality
evidence
• Limitations or special strengths can modify the quality of the evidence
44.
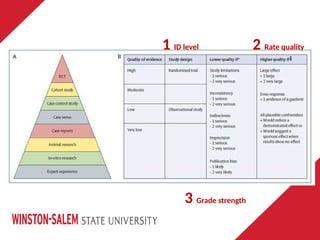
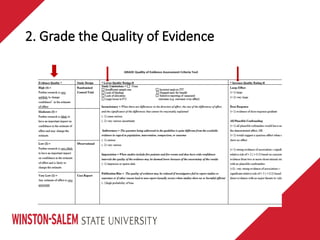
GRADE
1. Identify thelevel of evidence
2. Rate the quality of evidence (for each outcome)
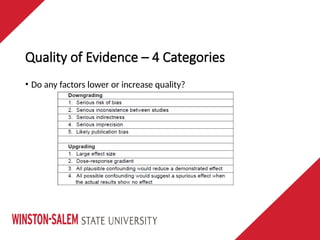
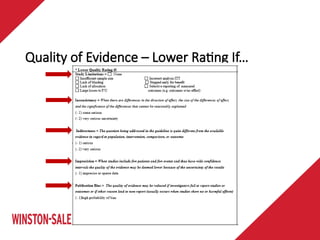
a. Do any factors lower quality?
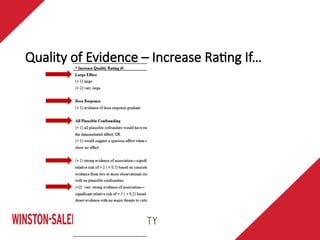
b. Do any factors increase quality?
3. Grade strength of the recommendation
a. Do any domains contribute to strength?
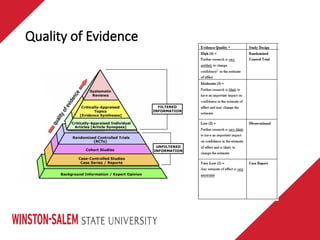
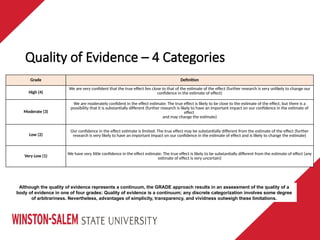
Quality of Evidence– 4 Categories
Grade Definition
High (4)
We are very confident that the true effect lies close to that of the estimate of the effect (further research is very unlikely to change our
confidence in the estimate of effect)
Moderate (3)
We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a
possibility that it is substantially different (further research is likely to have an important impact on our confidence in the estimate of
effect
and may change the estimate)
Low (2)
Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect (further
research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate)
Very Low (1) We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect (any
estimate of effect is very uncertain)
Although the quality of evidence represents a continuum, the GRADE approach results in an assessment of the quality of a
body of evidence in one of four grades: Quality of evidence is a continuum; any discrete categorization involves some degree
of arbitrariness. Nevertheless, advantages of simplicity, transparency, and vividness outweigh these limitations.
50.
Quality of Evidence– 4 Categories
• Do any factors lower or increase quality?
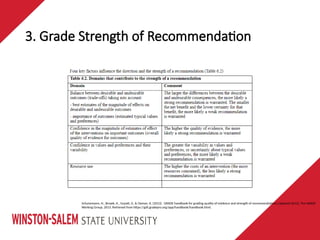
3. Grade Strengthof Recommendation
Schunemann, H., Brozek, K., Guyatt, G. & Oxman, A. (2013). GRADE handbook for grading quality of evidence and strength of recommendations {updated 2013}. The GRADE
Working Group, 2013. Retrieved from https://gdt.gradepro.org/app/handbook/handbook.html.
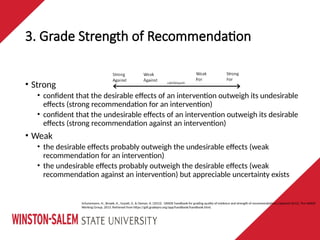
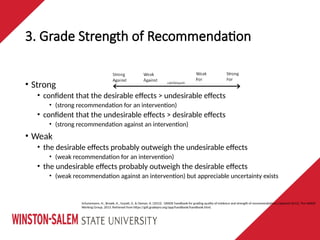
• Strong
• confident that the desirable effects of an intervention outweigh its undesirable
effects (strong recommendation for an intervention)
• confident that the undesirable effects of an intervention outweigh its desirable
effects (strong recommendation against an intervention)
• Weak
• the desirable effects probably outweigh the undesirable effects (weak
recommendation for an intervention)
• the undesirable effects probably outweigh the desirable effects (weak
recommendation against an intervention) but appreciable uncertainty exists
54.
3. Grade Strengthof Recommendation
Schunemann, H., Brozek, K., Guyatt, G. & Oxman, A. (2013). GRADE handbook for grading quality of evidence and strength of recommendations {updated 2013}. The GRADE
Working Group, 2013. Retrieved from https://gdt.gradepro.org/app/handbook/handbook.html.
• Strong
• confident that the desirable effects > undesirable effects
• (strong recommendation for an intervention)
• confident that the undesirable effects > desirable effects
• (strong recommendation against an intervention)
• Weak
• the desirable effects probably outweigh the undesirable effects
• (weak recommendation for an intervention)
• the undesirable effects probably outweigh the desirable effects
• (weak recommendation against an intervention) but appreciable uncertainty exists
55.
3. Grade Strengthof Recommendation
Schunemann, H., Brozek, K., Guyatt, G. & Oxman, A. (2013). GRADE handbook for grading quality of evidence and strength of recommendations {updated 2013}. The GRADE
Working Group, 2013. Retrieved from https://gdt.gradepro.org/app/handbook/handbook.html.
56.
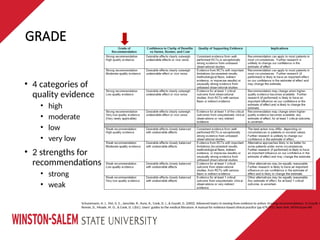
GRADE
Schunemann, H. J.,Vist, G. E., Jaeschke, R., Kunz, R., Cook, D. J., & Guyatt, G. (2002). Advanced topics in moving from evidence to action: Grading recommendations. In Guyatt, G
Rennie, D., Meade, M. O., & Cook, D. J.(Ed.), Users’ guides to the medical literature: A manual for evidence-based clinical practice (pp 679-701). New York, NY:McGraw-Hill.
• 4 categories of
quality evidence
• high
• moderate
• low
• very low
• 2 strengths for
recommendations
• strong
• weak
57.
GRADE
Guyatt, G,, Oxmanc,A., Akl, E., Kunz, R., Vist, G, Brozek…Sch€unemann, H. (2011). GRADE guidelines: Introduction GRADE evidence profiles and summary of findings tables.
Journal of Clinical Epidemiology 64(2011), 383-394. Retrieved from https://www.jclinepi.com/article/S0895-4356(10)00330-6/fulltext
58.
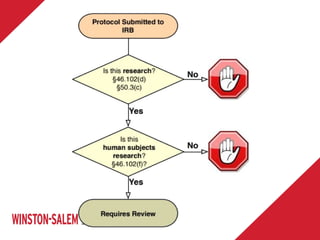
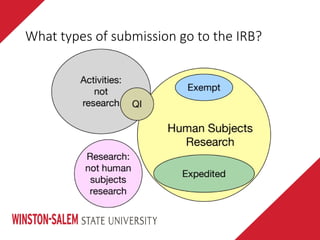
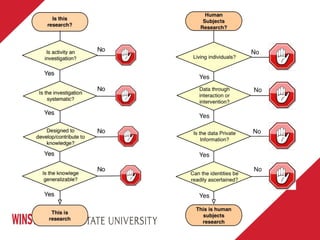
IRB & QI:Is This Human
Subjects Research?
Adapted from AHRQ Is this QI or Human Subjects Research?
Implications for Practice-Based Research
60.
• “Quality improvementefforts are held up by uncertainties about
when and how IRB review should be done.”
Clinical Infectious Diseases 2009;49:328–35
61.
• “QI isan integral part of good clinical practice and is designed to
bring about immediate improvements in health care in local
settings. In contrast, …human subjects research is not a necessary,
integral element of good clinical practice and that human subjects
research aims to generate new, generalizable, and enduring
knowledge about human health.”
• However - can be overlap between the two
Ann Intern Med. 2007;146:680-681
62.
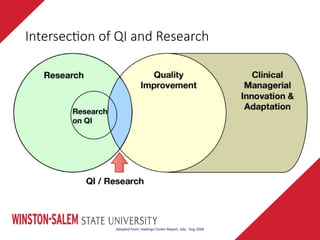
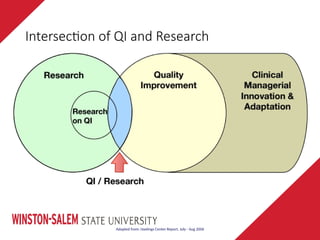
Intersection of QIand Research
Adapted from: Hastings Center Report, July - Aug 2006
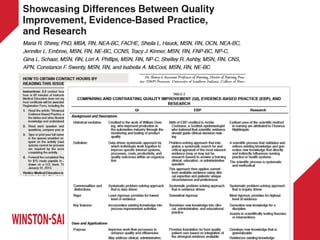
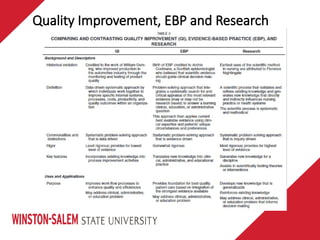
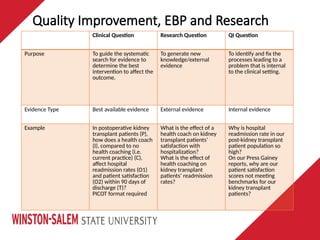
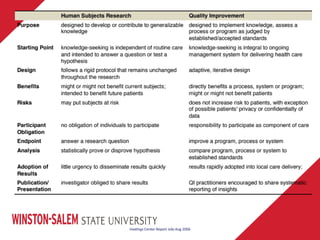
Quality Improvement, EBPand Research
Clinical Question Research Question QI Question
Purpose To guide the systematic
search for evidence to
determine the best
intervention to affect the
outcome.
To generate new
knowledge/external
evidence
To identify and fix the
processes leading to a
problem that is internal
to the clinical setting.
Evidence Type Best available evidence External evidence Internal evidence
Example In postoperative kidney
transplant patients (P),
how does a health coach
(I), compared to no
health coaching (i.e.
current practice) (C),
affect hospital
readmission rates (O1)
and patient satisfaction
(O2) within 90 days of
discharge (T)?
PICOT format required
What is the effect of a
health coach on kidney
transplant patients’
satisfaction with
hospitalization?
What is the effect of
health coaching on
kidney transplant
patients’ readmission
rates?
Why is hospital
readmission rate in our
post-kidney transplant
patient population so
high?
On our Press Gainey
reports, why are our
patient satisfaction
scores not meeting
benchmarks for our
kidney transplant
patients?
67.
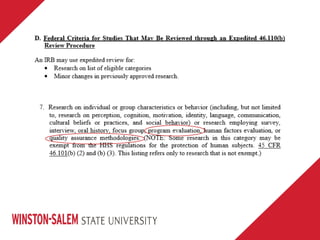
Aim is todevelop QI/EBP project in a manner that determines it to be exempt or expedited
• Exempt category 3
• Expedited category 7
71.
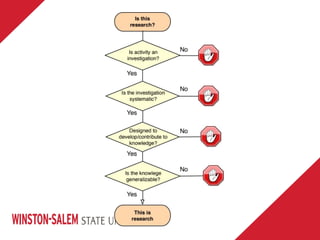
Research: Regulatory Definition
•Research means a systematic investigation, including research
development, testing and evaluation, designed to develop or
contribute to generalizable knowledge.
• Research is a set of behaviors or processes not an outcome
• Many systematic activities are not research (QI)
• Generalizable knowledge is an outcome that can result from many non-
research activities
45 CFR 46.102(d)
72.
Research versus Practice
•“Research is usually described in a formal protocol that sets forth an
objective and a set of procedures designed to reach that objective.”
• Employ research methodology (e.g. randomization)
• Obligation is to adhere to protocol rather than individualization of care
• Benefit to future patients, knowledge
Belmont Report, 1979
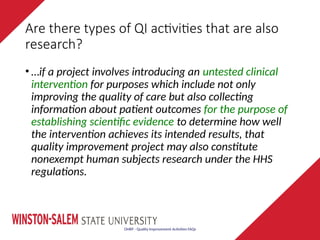
Are there typesof QI activities that are also
research?
• …if a project involves introducing an untested clinical
intervention for purposes which include not only
improving the quality of care but also collecting
information about patient outcomes for the purpose of
establishing scientific evidence to determine how well
the intervention achieves its intended results, that
quality improvement project may also constitute
nonexempt human subjects research under the HHS
regulations.
OHRP - Quality Improvement Activities FAQs
76.
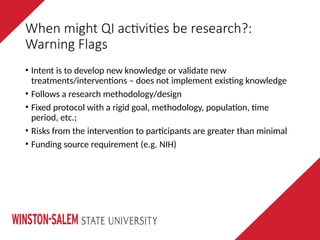
When might QIactivities be research?:
Warning Flags
• Intent is to develop new knowledge or validate new
treatments/interventions – does not implement existing knowledge
• Follows a research methodology/design
• Fixed protocol with a rigid goal, methodology, population, time
period, etc.;
• Risks from the intervention to participants are greater than minimal
• Funding source requirement (e.g. NIH)
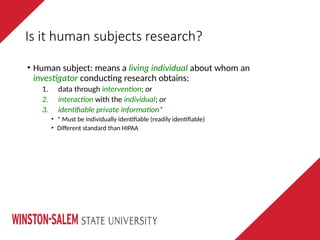
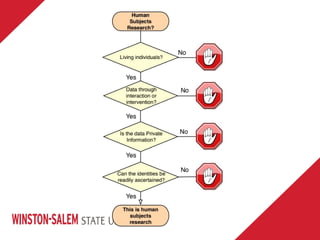
Is it humansubjects research?
• Human subject: means a living individual about whom an
investigator conducting research obtains:
1. data through intervention; or
2. interaction with the individual; or
3. identifiable private information*
• * Must be individually identifiable (readily identifiable)
• Different standard than HIPAA
81.
IRB & QIDiscussion
Panel:
Is This Human Subjects
Research?
Panelists:
Vernon Shanks, Associate Director, Office of Sponsored
Programs
Islam Khan, PhD, Compliance Officer, Office of Sponsored
Programs
82.
Intersection of QIand Research
Adapted from: Hastings Center Report, July - Aug 2006
84.
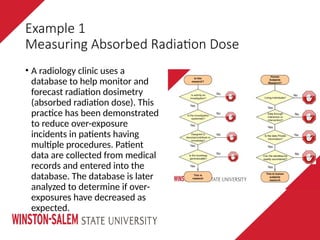
Example 1
Measuring AbsorbedRadiation Dose
• A radiology clinic uses a
database to help monitor and
forecast radiation dosimetry
(absorbed radiation dose). This
practice has been demonstrated
to reduce over-exposure
incidents in patients having
multiple procedures. Patient
data are collected from medical
records and entered into the
database. The database is later
analyzed to determine if over-
exposures have decreased as
expected.
85.
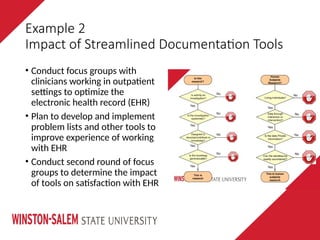
• Conduct focusgroups with
clinicians working in outpatient
settings to optimize the
electronic health record (EHR)
• Plan to develop and implement
problem lists and other tools to
improve experience of working
with EHR
• Conduct second round of focus
groups to determine the impact
of tools on satisfaction with EHR
Example 2
Impact of Streamlined Documentation Tools
86.
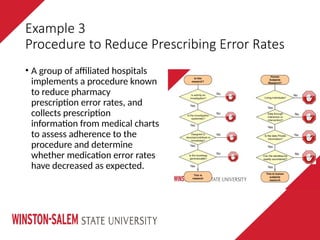
Example 3
Procedure toReduce Prescribing Error Rates
• A group of affiliated hospitals
implements a procedure known
to reduce pharmacy
prescription error rates, and
collects prescription
information from medical charts
to assess adherence to the
procedure and determine
whether medication error rates
have decreased as expected.
87.
Example 4
Trial toImprove Outpatient Asthma Care
• Practices will be cluster
randomized to a multipart
intervention including education,
EHR decision support, and
receipt of spirometers
• The objectives are to determine if
the intervention improves
patients’ asthma outcomes
• Data from all physicians’ patients
with asthma meeting age criteria
will be included
88.
Example 5
Implementing CapacityAssessments
• A clinic … implements a widely
accepted capacity assessment as
part of routine standard of care in
order to identify patients requiring
special services and staff expertise.
The clinic expects to audit patient
charts in order to see if the
assessments are performed with
appropriate patients, and will
implement additional in-service
training of clinic staff … if it finds
that the assessments are not being
administered routinely.
89.
• Objectives areto decrease the rate
of clotted or insufficient samples
for outpatient blood tests. The
intent is to improve family
satisfaction by decreasing the
need to repeat lab tests
• Plan to look at existing and
prospective records to examine
the timing of procedures and
method of blood draw (i.e., finger
stick or needle stick)
Example 6
Improving the Process of Drug Monitoring
90.
Example 7
Parent SatisfactionSurvey with Fast Track Clinic
• The purpose of the survey is to
determine the parent's
satisfaction with the staff,
healthcare provider, and care
• Providers will note the child’s
diagnosis, time spent for the
visit, and comment on whether
or not the child met the "Fast
Track Clinic" criteria
• The intent is to improve triage of
patients and to improve parent
satisfaction with care
91.
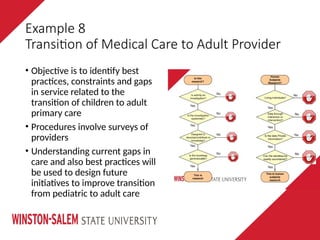
Example 8
Transition ofMedical Care to Adult Provider
• Objective is to identify best
practices, constraints and gaps
in service related to the
transition of children to adult
primary care
• Procedures involve surveys of
providers
• Understanding current gaps in
care and also best practices will
be used to design future
initiatives to improve transition
from pediatric to adult care
92.
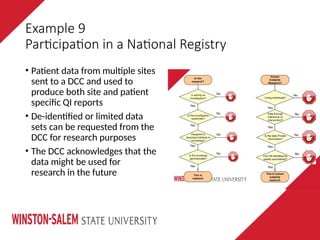
Example 9
Participation ina National Registry
• Patient data from multiple sites
sent to a DCC and used to
produce both site and patient
specific QI reports
• De-identified or limited data
sets can be requested from the
DCC for research purposes
• The DCC acknowledges that the
data might be used for
research in the future
93.
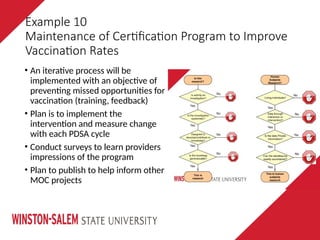
• An iterativeprocess will be
implemented with an objective of
preventing missed opportunities for
vaccination (training, feedback)
• Plan is to implement the
intervention and measure change
with each PDSA cycle
• Conduct surveys to learn providers
impressions of the program
• Plan to publish to help inform other
MOC projects
Example 10
Maintenance of Certification Program to Improve
Vaccination Rates
#10 assignments provide opportunity for application
allowed a full week of no other assignments in this class to allow focus on what is due; do not start weekend or day of; this is not that kind of work
#12 Develop skills to search the literature and be better informed re the problem in the population; not about regurgitation, but analysis, evaluation and synthesis
Reverse outline / main idea and supporting details
Format/APA (Writing center)
Abstract at the end
Alignment
Quality indicator
Relevant/Pertinent/Inform problem in population
#13 Share the priority opportunity for improvement with revision re problem in population? Where are you stuck?
Answer each other
#14 Why are you reviewing the literature? To summarize and synthesize evidence about the problem (will evolve to include solution/intervention)
#16 Clinical Question (PICOT)
practice vs research
#17 Clinical question/PICOT
what is everyone’s PICOT question? Let’s discuss
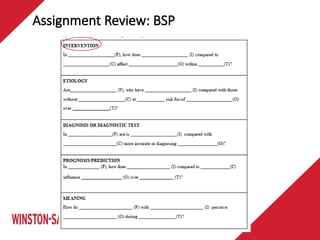
Sample Questions:
Intervention: In African-American female adolescents with hepatitis B (P), how does acetaminophen (I) compared to ibuprofen (C) affect liver function (O)?
Etiology: Are 30- to 50-year-old women (P) who have high blood pressure (I) compared with those without high blood pressure (C) at increased risk for an acute myocardial infarction (O) during the first year after hysterectomy (T)?
Diagnosis: In middle-aged males with suspected myocardial infarction (P), are serial 12-lead ECGs (I) compared to one initial 12-lead ECG (C) more accurate in diagnosing an acute myocardial infarction (O)?
Prognosis/Prediction: 1) For patients 65 years and older (P), how does the use of an influenza vaccine (I) compared to not receiving the vaccine (C) influence the risk of developing pneumonia (O) during flu season (T)?
2) In patients who have experienced an acute myocardial infarction (P), how does being a smoker (I) compared to a non-smoker (C) influence death and infarction rates (O) during the first 5 years after the myocardial infarction (T)?
Meaning: How do 20-something males (P) with a diagnosis of below the waist paralysis (I) perceive their interactions with their romantic significant others (O) during the first year after their diagnosis (T)?
#26 Transparent, not jumping from 2345 to 10 b/c only focus on unique population
scholarly, publication worthy
Who used the librarian?
#27 best to have some kind of way to organize your search
was not required but now suggest
Who used the librarian?
#28 If you were to appraise your writing so far according to the criteria you are learning about, what opportunities do you have for improvement?
Grove text, chapter 6
#29 This was about how to rapidly and critically appraise and determine if something was a keeper or not; reasonable that would find some and indicate not; also to identify if relevant and if answered the PICOT question, and what are implications? Can I use this?
Essentially testing understanding of research design content covered in weekly course content because you had to ID the evidence type and be able to identify the components you were looking for in order to answer the questions
Where did you get stuck?
#31 Should be gathering literature to support intervention, consider RCA questions, consider implications, etc
#32 These assignments feed into each other
Background and sig paper
write/share current knowledge of the problem
get in the literature!
(get feedback)
Rapid Critical Appraisals
Look at Interventions that claim to solve the problem and evaluate if they are solutions and evaluate if credible
ID at least 3 interventions of interest
(feedback)
Evaluation Tables
further analyze keeper studies for 3 interventions
IMPORTANT as use these to support the intervention you select to implement and often will replicate your study from
get in the literature!
level of evidence, quality of evidence = strength of recommendation to use and change practice (subjective, be able to provide rationale)
(feedback)
Evidence Synthesis Table
group, compare, contrast
ID strengths, weaknesses, differences
Synthesis!!!!!
(feedback)
EBP Paper
write up what found in synthesis table
ID intervention with strongest evidence
Consider feasibility to practice site
(feedback)
Seminar presentation
current knowledge re problem
review of interventions, quality, one with strongest evidence
(feedback)
Literature Review
final write up
(incorporate feedback from Bkgrnd/Sig and EBP)
#33 Everything you do builds towards your DNP Project or Scholarly Project
Proposal slides or poster
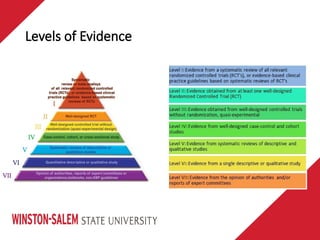
#38 you are aware of levels of evidence
give more definition to quality
learn about strength of evidence
#40 The higher the hierarchy, the higher the quality of evidence
the lower the hierarchy, the lower the quality of evidence
#45 Identify the level of evidence
Rate the quality of evidence (for each outcome)
Do any factors lower quality?
Do any factors increase quality?
Grade strength of the recommendation
Do any domains contribute to strength?
#59 Everyone has this article with this table.
Take a moment to look over the differences between QI, EBP and research.
Tell me what is different.
#63 QI = bright idea
EBP = EBP, generate new kevidence
Research = new knowledge, not asked before
#64 QI = bright idea
EBP = EBP, generate new evidence
Research = new knowledge, not asked before
#67 Exempt does not require full board review and gets through quicker; PI has been clear and it is easy for CO to determine if it is straightforward
Expeditable does not require full board review
All others get full board review
Various categories of exempt and expedited
#68 QI/Program evaluation
Aggregate data (de-identified), no direct interaction with participants
#69 Exempt does not require full board review and gets through quicker; PI has been clear and it is easy for CO to determine if it is straightforward
Expeditable does not require full board review
All others get full board review
Various categories of exempt and expedited















































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)










