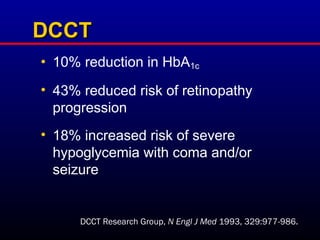
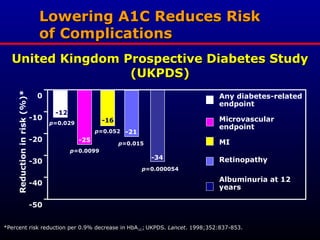
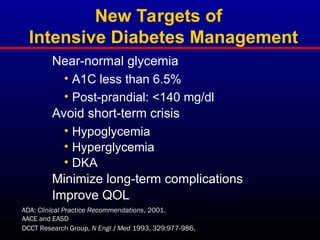
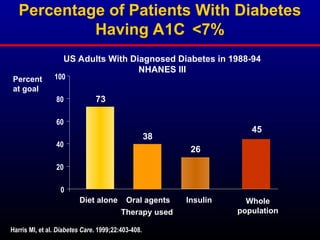
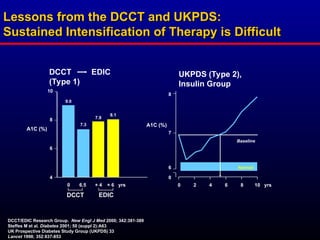
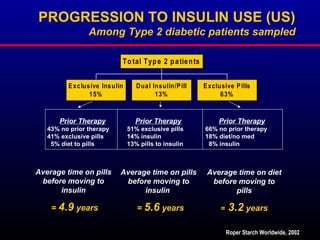
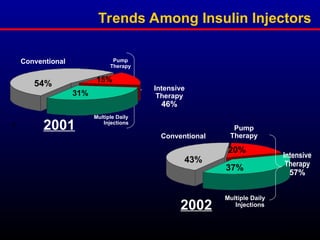
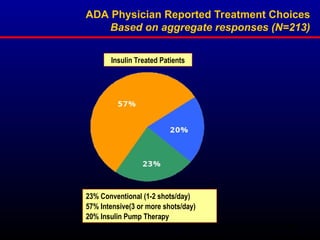
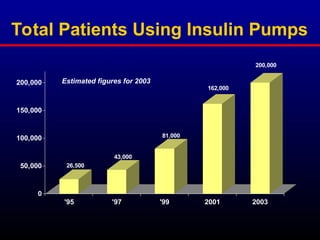
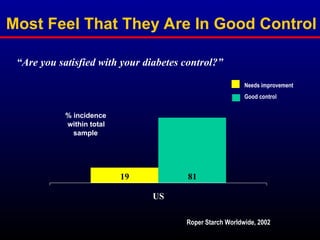
Diabetes prevalence and associated costs continue to rise globally, with lower treatment targets promoting the adoption of more intensive management strategies. The use of intensive insulin management, including insulin pumps, is increasing among patients, despite barriers such as patient perceptions of control. Overall, there is a notable trend towards improved diabetes management, though many patients may still lack awareness of their condition's seriousness.