Escort Service Call Girls In Sarita Vihar,, 99530°56974 Delhi NCR
Development of respiratory system
1. DEVELOPMENT OF RESPIRATORY SYSTEM
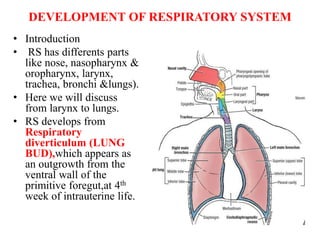
• Introduction
• RS has differents parts
like nose, nasopharynx &
oropharynx, larynx,
trachea, bronchi &lungs).
• Here we will discuss
from larynx to lungs.
• RS develops from
Respiratory
diverticulum (LUNG
BUD),which appears as
an outgrowth from the
ventral wall of the
primitive foregut,at 4th
week of intrauterine life.
3. IMPORTANT POINTS
( for spotter)
• Respiratory system is ENDODERMAL in origin.
• RS develops from RESPIRATORY DIVERTICULUM >
(LUNG BUD).
• Lungs develop from Lung bud.
• RS develops at 4th week of IUL.
• Factors responsible for development of RS are
1> Retinoic acid –produced by adjacent mesoderm
• 2> Transcription factor TBX4 – present in endoderm of
GUT TUBE (GIT)
• LINING EPITHELIUM of LARYNX,TRACHEA
,BRONCHI & LUNG is derived from ENDODERM
• CARTILAGES,MUSCLES & CONNECTIVE TISSUE
OF RS is derived from SPLANCHNIC MESODERM
surrounding the foregut.
4. FORMATION OF LUNG BUD/RESPIRATORY
DIVERTICULUM/LARYNGOTRACHEAL
DIVERTICULUM• This diverticulum is 1st seen as a midline groove called
Laryngotracheal groove in the endodermal lining of primitive
pharynx just caudal to hypobronchial eminence during 4th week
of IUL.
• The groove deepens to form a longitudinal diverticulum called
Laryngotracheal diverticulum which is in open communication
with the foregut.
As the LD expand caudally, two longitudinal ridge/fold called
Tracheoesophageal ridge develop that grow medially & fuse to
form septum called Tracheoesophageal septum, which separates
the distal part of LD from foregut (esophagus).whereas the cranial
part continues to communicate with pharynx. This communication
with pharynx forms Laryngeal inlet.
The separated part of LD grows downwards to enter thorax & form
TRACHEA & Rt.& Lt. BRONCHIAL BUD.
The cranial most part of LD gives development of LARYNX.
Each bronchial bud invaginates into Pericardioperitoneal canal .This
canal forms the pleural cavities.
5. FORMATION OF LUNG BUD/RESPIRATORY
DIVERTICULUM/LARYNGOTRACHEAL
DIVERTICULUM
• a midline groove called
Laryngotracheal groove
• The groove deepens to form
a longitudinal diverticulum
( Laryngotracheal
diverticulum)/ [LD]
• Which is in open
communication with the
foregut.
• Tracheoesophageal ridge
develop from side
• form septum called
Tracheoesophageal septum,
• which separates the distal part
of LD from foregut
(esophagus).
• But communicates with
pharynx through Laryngeal
inlet.
• The separated part of LD
grows downwards to enter
thorax & form TRACHEA &
Rt.& Lt. BRONCHIAL
BUD.
• The cranial most part of LD
gives development of
LARYNX.
7. • Introduction
• RS is divided into URT (nose,nasopharynx &
oropharynx) and LRT (larynx,trachea,bronchi
&lungs).
• Here we will discuss about LRT.
• RS develops from Respiratory diverticulum
(LUNG BUD),which appears as an outgrowth
from the ventral wall of the primitive
foregut,at 4th week of intrauterine life.
DEVELOPMENT OF LARYNX & REVIEW
OF FORMATION OF RESPIRATORY
DIVERTICULUM// LARYNGO-TRACHEAL
DIVERTICULUM
8. .• The larynx develops from the cranial most part of the Laryngotracheal
diverticulum.
• The communication between the laryngotracheal diverticulum & primitive
pharynx persists as Laryngeal inlet .
• The internal lining of larynx originates from Endoderm, & all the cartilages
(except Epiglottis) & muscles originates from 4th & 6th pharyngeal arches.
• The epiglottis develop from the caudal part of Hypobronchial eminence.
• Since vagus is the nerve of 4th & 6th pharyngeal arch. Hence superior
laryngeal nerve innervates derivatives of 4th pharyngeal arch, Recurrent
Laryngeal nerve innervates derivatives of 6th pharyngeal arch.
• During development, proliferation of mesenchyme form cartilages like
thyroid,cricoid,arytenoid , & laryngeal inlet become T-shaped ,on the
other hand , rapid proliferation of endodermal cells (of lining epithelium)
obliterate the lumen of larynx temporarily. Later on the cells obliterating
the lumen breakdown and recanalization of larynx takes place .during
recanalization , the endodermal cells form two pair of folds ,which extends
antero-posteriorly in the lumen of larynx , the upper pair is vestibular fold
and lower pair is vocal fold and give rise to False & True vocal cord
respectively.
• A pair of lateral recesses bounded by these folds is called Laryngeal
ventricles.
9. Nerve supply of larynx
• All intrinsic muscles of larynx except
cricothyroid is supplied by recurrent laryngeal
while cricothyroid by external laryngeal nerve.
• Sensory supply- internal laryngeal nerve
supplies the mucous membrane above the true
vocal cord and Recurrent laryngeal nerve
supplies mucosa below the level the vocal
cord.
14. DEVELOPMENT OF LARYNX &
REVIEW OF FORMATION OF
RESPIRATORY DIVERTICULUM//
LARYNGO-TRACHEAL
DIVERTICULUM
• .
15. LARYNGO-TRACHEAL GROOVE
IN PRIMITIVE FOREGUT(caudal
part of pharynx),Distal to
hypobronchial eminence
• .
LARYNGOTRACHEAL DIVERTICULUM (
LD) (communicating with primitive foregut)
TRACHEO-ESOPHAGEAL RIDGE / FOLD
TRACHEO-ESOPHAGEAL SEPTUM
SEPARATION OF “LD”
DISTAL PART OF LD GET SEPARATED
FROM PRIMITIVE FOREGUT
(ESOPHAGUS), BUT CRANIAL PART
REMAINS IN CONTINUITY WITH
FOREGUT (CAUDAL PART OF
PHARYNX)
THIS CONTINUITY FORMS
LARYNGEAL INLET (SLIT LIKE ) &
CRANIAL PART OF “ LD” FORMS
LARYNX.
i.e.
Larynx develop from
cranial most part of the
laryngo-tracheal diverticulum
(lung Bud)
18. LARYNX
Cartilage & muscle of larynx ,originate
from mesenchyme of 4th &6th pharyngeal
arches
• Mesenchyme proliferate rapidly & form
laryngeal cartilages like-
thyroid,cricoid&arytenoid and these
cartilages change the shape of laryngeal
inlet from slit like to T-shaped.
* EPIGLOTTIS develop from caudal part
of Hypobronchial eminence.
NERVE SUPPLY OF LARYNX-by nerve
of 4th & 6th Ph.Arches –vagus.
1> superior laryngeal nerve supply
derivatives of 4th ph. Arch
2> Recurrent laryngeal nerve innervates
derivative of 6th ph. Arch.
Internal lining of Larynx
• Originates from Endoderm
• This lining epithelium proliferates
rapidly & temporarily close the
lumen of the Larynx.
• Then vacuolization &
recanalization occur
• As a result a pair of lateral
recesses (space) formed, called
Laryngeal ventricle.
• These recesses are bounded by
folds of tissue called Vestibular
fold & vocal fold, that form false
and true vocal cord respectively.
19. APPLIED RELATED TO
DEVELOPMENT OF LARYNX
• 1>Laryngeal atresia & stenosis- d/t failure of
recanalization of larynx , leading to obstruction of URT.it is
also called congenital high airway obstruction syndrome.
• 2>Laryngeal web- an abnormal membranous ,web like
tissue is present in the lumen of larynx , near the vocal fold.
This also partially obstruct the airway.
• 3>One or more laryngeal cartilage may be absent.
• 4>MAY BE DOUBLE LARYNX OR SOME PART OF IT
MAY BE DOUBLE
• 5>LARYNGOPTOSIS- the larynx lies at lower level , it
may lies behind the sternum.
• 6>LARYNCOELE- In this condition the laryngeal saccule
(ventricles) is abnormally large & forms swelling in the
neck.
20. APPLIED RELATED TO
DEVELOPMENT OF LARYNX
• 1>Laryngeal atresia & stenosis- d/t failure of
recanalization of larynx , leading to obstruction of URT.it is
also called congenital high airway obstruction syndrome.
• 2>Laryngeal web- an abnormal membranous ,web like
tissue is present in the lumen of larynx , near the vocal fold.
This also partially obstruct the airway. This web like tissue
is derived from endodermal cells that fail to break out
during recanalization.
• 3>One or more laryngeal cartilage may be absent.
• 4>MAY BE DOUBLE LARYNX OR SOME PART OF IT
MAY BE DOUBLE
• 5>LARYNGOPTOSIS- the larynx lies low down in the
neck,some part of it may lies behind the sternum.
• 6>LARYNCOELE- In this condition the laryngeal saccule
(ventricles) is abnormally large and may extend beyond the
larynx proper & forms swelling in the neck.
21. DEVELOPMENT OF TRACHEA
• The trachea develops from the part of
Laryngotracheal diverticulum(respiratory
diverticulum), which lies between the Larynx
and point of division of LTdiv. Into
Bronchial buds.
• Lining epithelium derived from Endoderm.
• Cartilage,muscle and connective tissue of
trachea splanchno-pleuric mesoderm
surrounding laryngotracheal groove.
22. APPLIED RELATED TO
DEVELOPMENT OF TRACHEA
• TRACHEOESOPHAGEAL FISTULA
(TEF)- abnormal communication between
trachea and esophagus
• Tracheal stenosis or narrowing of trachea
• Tracheal atresia or tracheal obstruction
• Tracheal bronchus and tracheal lobe-
sometimes trachea presents a diverticulum that
may end blindly or may bear a lobe.
23. TRACHEOESOPHAGEAL FISTULA
• It is abnormal communication between trachea & esophagus .
• It is usually associated with esophageal atresia (obstruction)
• It is due to defective development of tracheoesophageal septum
• TYPES
• 1> upper end of esophagus ends in a blind pouch and lower part communicates with trachea
(most common type of TEF, 90%)
• 2> H-shaped TEF- both upper & lower part of the esophagus communicate with trachea by a
narrow canal near bifurcation of trachea,making a shape of “H”
• 3> upper part of esophagus communicates with trachea and lower end forms a blind pouch
• 4> both upper and lower part of esophagus communicate with trachea separately.
• C/F- if milk or fluid is given to newborn with TEF ,there will be coughing & choking ,d/t
entery of milk in respiratory tract. May lead to lung infection or pneumonia.
• Complication of TEF is POLYHYDRAMINOS because in some type of TEF amniotic fluid
does not pass to the stomach& intestine of fetus.
• TEFs are a component of VACTERL association---Vertebralanomalies,Anal atresia,Cardiac
defects,Tracheoesophageal fistula,Esophageal atresia , Renal anomalies ,and Limb defect.
24.
25. QUESTION
• A prenatal USG revealed polyhydraminos, and at birth
the baby had excessive fluids in its mouth. What type of
birth defect might be present, and what is its
embryological origin? Would you examine the child
carefully for other birth defects? Why? [ 4
marks]
• ANS- TEF with esophageal atresia / tracheoesophageal
atresia with or without TEF
• Due to defective tracheoesophageal septum
• Examine for other anomalies of VACTERL association,
because tracheoesophageal atresia is a component of
VACTERL association.
26. DEVELOPMENT OF BRONCHUS AND LUNG
• The respiratory diverticulum divides into two bronchial buds.
• Each bronchial bud develops into a principal bronchus i.e.Lt. & Rt.
Primary/principal bronchus formed.
• The principal bronchi divide to form secondary bronchi ,three sec. Bronchi on Rt.
Side & two sec. Bronchi on Lt. Side is formed (hence 3 lobes present in Rt.lung &
2 lobes in Lt.lung) .
• During further development secondary bronchi divide repeatedly in dichotomous
fashion, forming 10 tertiary (segmental) bronchi in each lung (hence 10
bronchopulmonary segments present in each lung)
• By the end of 6th month 17 generations of subdivision occur in bronchial tree.
Nearly 6 subdivision occur in post natal life to reach the final shape of bronchial
tree..
• Thus division & subdivisions of each segmental bronchus form the distal part of
bronchial tree consisting of Bronchioles,respiratory bronchioles,alveolar duct &
Alveoli.
• Alveoli is foemed by expansion of the terminal part of the bronchial tree.
• THUS— a) LUNGS PARENCHYMA derive from BRONHIAL TREE by several
subdivision of lobar bronchus. b)cartilages,smooth muscles ,& connective tissue
is derived from splanchnic mesoderm c) Lining epithelium of bronchial tree is
endoderm of respiratory diverticulum.
• LUNG BUD arise from foregut & as it grow ,it invaginates PERICARDIO-
PERITONEAL CANAL. In course of development ,lung bud form LUNG &
pericardio-peritonial canal form PLEURAL CAVITY after separating from
pericardial & peritoneal cavity.
• Since pleura lines the surface of each lobe separately, the lobes become separated
by fissures.
27. Development of bronchus
RESPIRATORY DIVERTICULUM
Right bronchial bud
• Rt. Principal bronchus/primary
bronchus
• Three secondary/ lobar bronchus
• Ten tertiary bronchus /segmental
bronchus
• 17 generation of subdivisions before
birth & 6 subdivisions after birth
• Terminal bronchiole ,respiratory
bronchiole,alveolar duct ,atria,, &
alveoli are formed
• Alveoli is formed by expansion of
terminal part of bronchial tree
Left bronchial bud
• Left principal
bronchus/primary bronchus
• Two secondary /lobar bronchus
• Ten tertiary/ segmental
bronchus
• 17 genertion of
subdivisions..........similar to rt.
lung
28.
29. Development of lung
• Lung Parenchyma – derived from bronchial
tree
• Lining epithelium – from endoderm of
resp.diverticulum
• Cartilages,muscle,& connective tissue –
from splanchnic mesoderm
30. APPLIED
• 1> Agenesis of lung
• 2> hypoplasia of lung
• 3> ectopic lung
• 4> abnormal lobes of lung– 2 in rt. & 3 in
left, due to abnormal division of principal
bronchus
• 5> congenital polycystic lung
• 6> azygos lobe of lung
31. APPLIED RELATED TO
DEVELOPMENT OF BRONCHUS &
LUNG• 1> agenesis of lung- one lung may be absent , if one bronchial bud
fails to develop.
• 2> Hypoplasia of lung – lungs are small & underdeveloped.
• 3> Ectopic lung-it may arise from esophagus or trachea, due to
additional/extra respiratory bud of trachea & foregut
• 4> Congenital polycystic lung- multiple cysts are formed in the
lung due to abnormal dilatation of terminal bronchioles, giving
HONEYCOMB appearance in radiograph.
• 5> Abnormal lobes of lung- sometimes Rt. Lung has two lobes
while Lt. Lung has three lobes , it is due to abnormal division of
principal bronchi into Lobar bronchi.
• 6> Azygos lobe of lung- normally upper lobe of Rt. Lung lies
lateral to the azygos vein but when a part of this lobe lies medial to
the azygos vein ,it forms the azygos lobe .
32. MATURATION OF LUNG
• It deals with histological & functional development of
the lung.
• Maturation of lung is divided into four stages-
1> Psuedoglandular stage- period- 5-16 weeks
of IUL
2> Canalicular stage- period 16-26 weeks of IUL
3> Terminal sac stage- period 26 week to birth
. (saccular stage)
4> Alveolar stage - period 8 month to childhood . .
. (8 Years)
35. 1- Pseudoglandular Period
(5-16 weeks)
• Developing lungs somewhat resembles an exocrine
gland during this period
• By 16 weeks all major elements of the lung have
formed except those involved with gas exchange
• (Terminal bronchioles are formed, BUT no
respiratory bronchioles or alveoli are present )
• Respiration is not possible at this stage
• Fetuses born during this period cannot survive
36. CANALICULAR STAGE
(16-26 Weeks)
• Each terminal bronchiole divide into 2 or more
Respiratory bronchiole
• Respiratory bronchiole divide into Alveolar
ducts.
• Lung is well vascularised
• Fetus born at this stage may or may not
survive.
37. TERMINAL SAC STAGE(saccular
stage)
( 26 weeks to Birth)• Large number of terminal sacs (primitive alveoli) are formed
• Capillaries bulge into the developing sacs
• Epithelium of terminal sac become very thin (simple squamous)
• Close contact develops between epithelium of sac & capillary to
permit adequate exchange of gases
• Fetus born at this stage survive
• Terminal sac lined mainly by type I alveolar epithelium(Type I
pneumocyte) & few type II alveolar epithelium (Type II
Pneumocyte)
• Type I pneumocyte (very thin or squamous epith.) take part in
gasseous exchange
• Type II pneumocytes secrete SURFACTANT that decrease surface
tension in alveoli.
38. ALVEOLAR STAGE
. (8month to 8 years)
32weeks to 8 years
• Formation of true alveoli more
&more(many)
• Many type II pneumocytes that produce
sufficient amount of surfactant
• Free exchange of gasses occur across the
blood-air barriers ( formed by epithelium of
alveoli and endothelium of capillaries).
39. APPLIED RELATED TO
MATURATION OF LUNG
• RESPIRATORY DISTRESS SYNDROME-
• Seen in premature newborn, due to insufficient
amount of SURFACTANT, So surface tension is high
leading to collapse of alveoli, as a result breathlessness
occur in newborn.
• In this disease ,alveoli of lungs are often filled with
fluid having high protein,which resembles glassy
hyaline membrane. Hence RDS is also k/a HYALINE
MEMBRANE DISEASE.
• NEWBORN with RDS is treated with either artificial
surfactant or glucocorticoids injection (which stimulate
surfactant production)
40. QUESTION
• A baby born at 6 months of gestation is having
trouble breathing. Why?
• Ans--- due to insufficient amount of
SURFACTANT, alveoli collapse—no gasseous
exchange occur
• Sufficient amount of surfactant is produced
after 7 month of IUL, ( alveolar stage)
41. Development of pleura
• After the formation of the head fold, the pericardium comes to lie on
the ventral aspect of the embryo , and the pericardio-peritoneal
canals wind backwards on either side of the foregut .
• The lung bud ,that arise from the foregut, now invaginate these
canals.
• As the bud enlarge to form the lungs, the canals balloon out to form
the pleural cavities
• Each pleural cavity now communicates with the pericardial cavity
through the pericardio-pleural opening and with the peritoneal
cavity through pleuro-peritonial opening
• Later on these openings are closed by formation of the pericardio-
pleural membrane & pleuro-peritoneal membrane respectively.