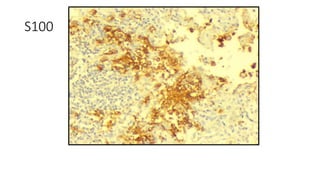
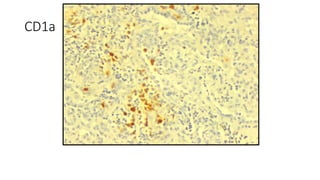
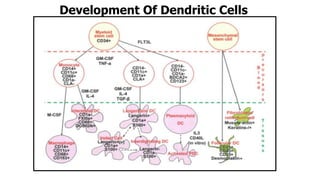
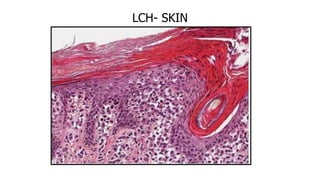
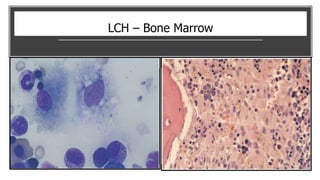
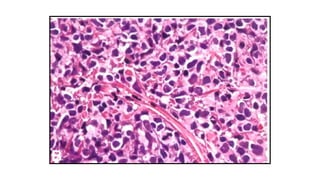
Dendritic cell tumors can arise from Langerhans cells or other dendritic cell subtypes. Langerhans cell histiocytosis (LCH) is characterized by proliferation of Langerhans cells and commonly involves bone, skin, lungs and lymph nodes. It ranges from localized eosinophilic granuloma to disseminated disease. Langerhans cell sarcoma is a rare malignant neoplasm that retains the immunophenotype of Langerhans cells. Indeterminate dendritic cell tumors have features intermediate between LCH and dendritic cell sarcoma.
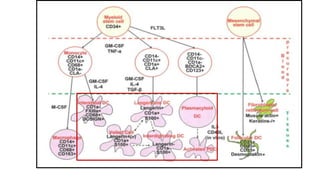

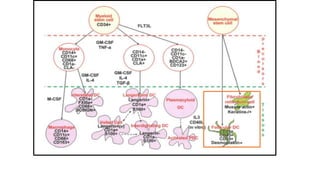



![HEMATOPOIETIC
STEM CELL (CD45+)
MESENCHYMAL
STEM CELL (CD45-)
PDC
FDC
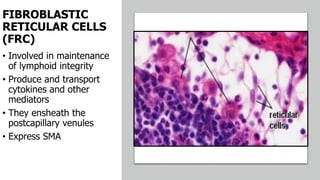
FRC
BPDCN
FRCT :
Indolent
to
aggressive
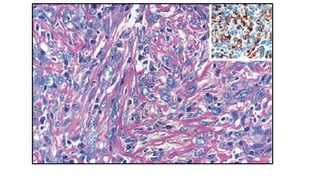
Spindle
cells with
collagen
fibres
IHC: SMA,
Desmin;
CK, CD68
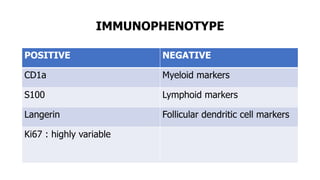
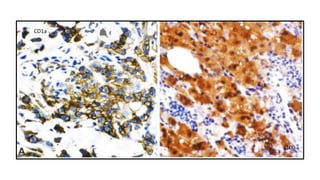
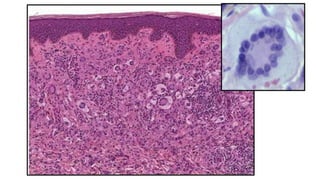
LCH:
Variable
clinical profile
LC cells
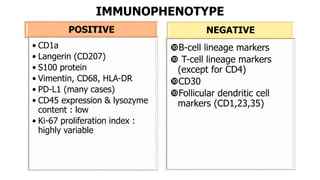
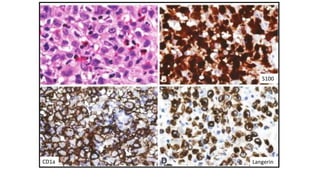
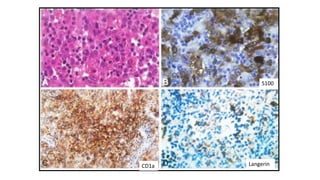
IHC: CD1a;
S100;Langerin
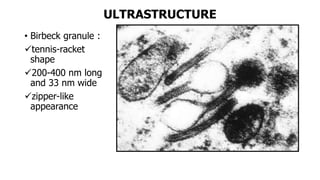
UM: Birbeck
granules
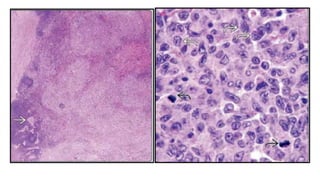
LCS:
aggressive
same IHC ;UM
ECD
DXG
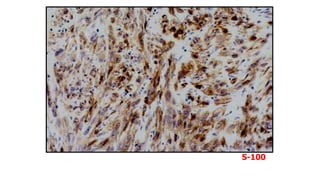
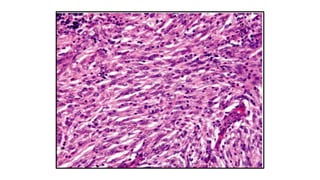
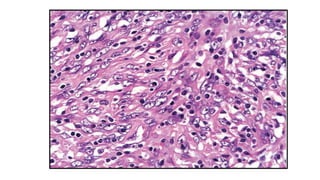
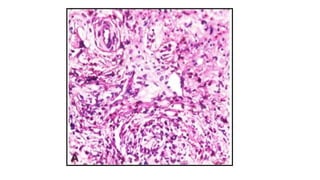
FDCS
:mostly LN,
mod
aggressive
Spindle cells
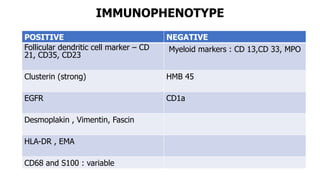
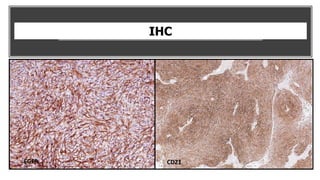
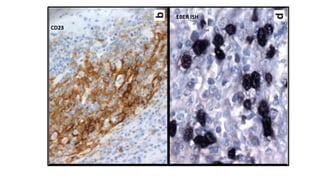
IHC:
CD21/35/23
Clusterin;
Fascin
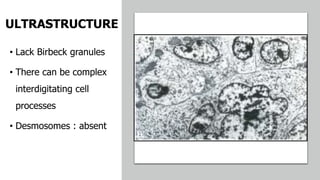
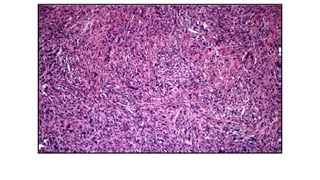
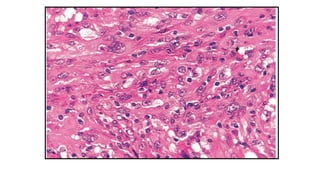
IDDCS : Mostly
LN; very
aggressive
Spindle cells
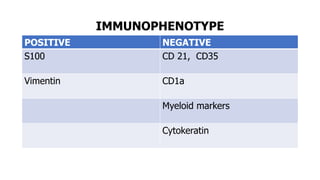
IHC : S100;
Fascin
Absent :CD1a,
Langerin
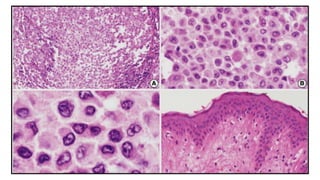
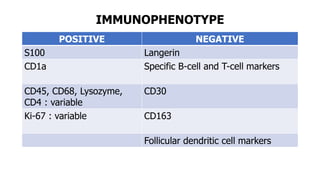
INDCT:
mostly localized
Oval cells
IHC:
CD1a;S100
Fascin
Absent : Langerin
Birbeck granules
–]-](https://image.slidesharecdn.com/subjectseminardendriticcells-190225131558/85/DENDRITIC-CELL-TUMORS-PATHOLOGY-133-320.jpg)