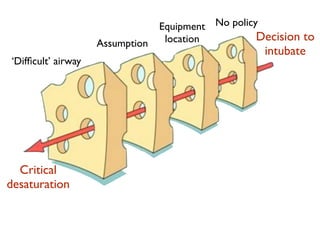
This document discusses crew resource management and communication in challenging medical environments. It emphasizes that medical professionals are human and fallible, that assumption can lead to mistakes, and the importance of open communication among the team. Some key points covered include acknowledging human limitations like stress, fatigue and ego; asking questions when unsure; speaking up if concerned; maintaining situational awareness; and not taking challenges personally as they are meant as a safety tool and for education. The overall message is that teamwork, communication and acknowledging human factors are vital for providing optimal patient care in high-pressure situations.










































































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

