Download as PDF, PPTX















![The care home resident population for those aged 65 and over has
remained almost stable since 2001 with an increase of 0.3%, despite
growth of 11.0% in the overall population at this age. Fewer women but
more men aged 65 and over, were living as residents of care homes in
2011 compared to 2001; the population of women fell by around 9,000
(-4.2%) while the population of men increased by around 10,000
(15.2%). The gender gap in the older resident care home population
has, therefore, narrowed since 2001. In 2011 there were around 2.8
women for each man aged 65 and over compared to a ratio of 3.3
women for each man in 2001. The resident care home population is
ageing: in 2011, people aged 85 and over represented 59.2% of the
older care home population compared to 56.5% in 2001. [Office of
National Statistics. Part of 2011 Census Analysis, Changes in the Older
Resident Care Home Population between 2001 and 2011 Release]
The total number of people receiving services in 2013-14 was 1,267,000
(down 5 per cent from 1,328,000 in 2012-13 and down 29 per cent from
1,782,000 in 2008-09). Of these, 1,046,000 received community based
services (a fall of 5 per cent from 2012-13), 204,000 received residential
care (a fall of 3 per cent from 2012-13) and 84,000 received nursing
care (which is 3 per cent down from 2011-12). [National Statistics.
Community Care Statistics, Social Services Activity, England - 2013-14,
Provisional release}](https://image.slidesharecdn.com/creativesupportinagedcare-141202002846-conversion-gate01/85/Creative-Support-in-Aged-Care-16-320.jpg)




![My Money
Funding from one
or more sources
[enables integration]
€
Coordinator Admin
Insurance Fund
brokerage overheads unexpected costs
Restricted Funding
Individual Service Fund](https://image.slidesharecdn.com/creativesupportinagedcare-141202002846-conversion-gate01/85/Creative-Support-in-Aged-Care-23-320.jpg)

























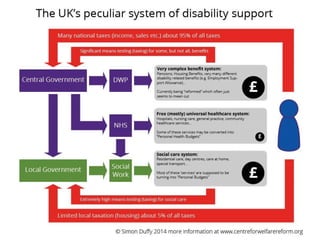
The document summarizes a workshop given by Dr. Simon Duffy on lessons from self-directed support in the UK. Duffy has 25 years of experience developing self-directed support systems and founded In Control, which developed the self-directed support model adopted in England. In the workshop, Duffy discusses the history and development of self-directed support in the UK, issues with current implementation, strengths to build on, and the importance of citizenship, community, and moving beyond concepts of consumers and care markets.















































































![Movie-Collection-Database.pptx[2].pptx for biotech](https://cdn.slidesharecdn.com/ss_thumbnails/movie-collection-database-260110184349-6042841d-thumbnail.jpg?width=640&height=640&fit=bounds)

