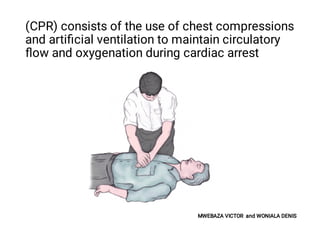
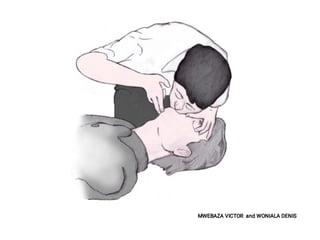
MWEBAZA VICTOR and WONIALA DENIS presented on cardiopulmonary resuscitation (CPR) to 5th year medical students at Kampala International University. CPR is an emergency procedure that combines chest compressions and artificial ventilation to preserve brain function and circulation in cardiac arrest. It involves chest compressions at a rate of 100-120 per minute and depth of 5-6 cm, as well as rescue breathing. Administration of electric shock through defibrillation is also sometimes needed to restore a viable heart rhythm for ventricular fibrillation or pulseless ventricular tachycardia. The goal of CPR is to maintain circulation and oxygenation until spontaneous circulation can be restored.