What isDiphtheria
Causative Agent: Corynebacterium diphtheriae
Transmission of Corynebacterium diphtheriae
Pathogenesis of Diphtheria
Virulence Factors of Corynebacterium diphtheriae
Clinical Features of Diphtheria
Diagnosis of Diphtheria
Laboratory Diagnosis Methods
Differential Diagnosis
Treatment of Diphtheria
Prevention of Diphtheria
3.
Diphtheria is abacterial infection caused by Corynebacterium diphtheriae.
It primarily affects the upper respiratory system,
such as the throat and nose, but it can also impact the skin and other parts of the
body.
The infection spreads through respiratory droplets when an infected person coughs
or sneezes.
DIPHTHERIA
4.
CAUSATIVE AGENT: CORYNEBACTERIUM
DIPHTHERIAE
▶1. Bacterial Characteristics:
• Gram-positive:
• Rod-shaped: It has a characteristic "club" or "picket-fence" appearance under the microscope.
• Non-spore forming
• Non motile
• Non capsulated
• Aerobic
• Slow-growing
▶ 2. Virulence Factor – Diphtheria Toxin:
The pathogenicity of Corynebacterium diphtheriae is largely due to the production of diphtheria toxin, a
potent exotoxin that is responsible for the symptoms and complications of the disease.
• Mechanism of Action: The diphtheria toxin interferes with protein synthesis in host cells by inactivating
the ribosome. This can lead to cell death, particularly in tissues like the throat and heart, causing
inflammation, tissue necrosis .
6.
TRANSMISSION OF CORYNEBACTERIUM
DIPHTHERIAE
▶Transmission of Corynebacterium diphtheriae primarily occurs through person-to-person contact, with
the following routes of transmission:
▶ 1. Airborne Droplets (Respiratory Transmission):
The incubation period for respiratory diphtheria is 2-5 days.
• Coughing and Sneezing: The most common mode of transmission is when an infected person coughs or
sneezes, releasing respiratory droplets containing the bacteria into the air. These droplets can be inhaled by
people nearby, leading to new infections.
• Close Contact: Prolonged close contact with an infected person, such as through kissing or sharing
utensils, can also facilitate transmission.
▶ 2. Contact with Contaminated Surfaces or Objects:
7.
• Skin Lesions:If a person has skin lesions infected with C. diphtheriae, the bacteria can be transmitted through direct
contact with the skin or lesions, though this is less common than respiratory transmission.
▶ 3. Carrier State:
• Asymptomatic Carriers: Some individuals who are infected with C. diphtheriae may not show symptoms but can still carry
the bacteria in their throat or nasal passages. These asymptomatic carriers can unknowingly spread the bacteria to
others, making control of the disease more challenging.
• Carriers are the more common source of infection than the cases itself ( 95%).
▶ 4. Less Common Modes of Transmission:
• Contact with Open Wounds: If someone comes into contact with an open wound or skin lesion from an infected
individual, transmission may occur, but this is more typical in cases of skin diphtheria.
8.
PATHOGENESIS OF DIPHTHERIA
▶The pathogenesis of diphtheria involves several key stages, including the entry of
Corynebacterium diphtheriae into the body, the production of diphtheria toxin, and
the resulting damage to tissues. Here's a detailed breakdown of how diphtheria
develops:
▶ 1. Entry of Corynebacterium diphtheriae into the Body:
• Corynebacterium diphtheriae typically enters the body through the respiratory tract
via
inhalation of infected respiratory droplets from coughing or sneezing by an infected
person.
• The bacteria can also enter through broken skin in cases of skin diphtheria, though
this is less common.
• Once the bacteria enter the body, they colonize the upper respiratory tract, which
includes the nose, throat (pharynx), tonsils, and larynx.
3
9.
▶ 2. Adherenceand Colonization:
• The bacteria use adhesins, which are proteins on the surface of C. diphtheriae, to adhere to the epithelial cells lining the
respiratory tract. This is a necessary step for colonization.
• C. diphtheriae grows and multiplies in the mucosal lining of the respiratory tract, producing a grayish pseudomembrane
made of dead cells, fibrin, and bacteria. This pseudomembrane is a hallmark sign of diphtheria and can obstruct the airway,
leading to breathing difficulties.
▶ 3. Production of Diphtheria Toxin:
• The key factor in the pathogenesis of diphtheria is the production of diphtheria toxin, a potent exotoxin that is responsible
for the majority of the damage caused by the disease.
• Diphtheria toxin is produced by C. diphtheriae only when the bacterium carries a tox gene, which it acquires through a
bacteriophage . The toxin is secreted into the surrounding tissues.
• The toxin acts by inhibiting protein synthesis in host cells, which leads to cell death. It primarily affects eukaryotic cells,
particularly in the throat, heart, nerves, and kidneys.
10.
1
5
▶ 4. Mechanismof Action of Diphtheria Toxin:
• Toxin Binding: The diphtheria toxin binds to a receptor on the surface of target cells (primarily epithelial cells in the
throat, but also heart and nerve cells).
• Endocytosis: After binding, the toxin is internalized by the host cell through endocytosis.
• Inhibition of Protein Synthesis: Once inside the cell, the toxin catalyzes the transfer of an ADP-ribose group to the
elongation factor-2 (EF-2), which is essential for protein synthesis in the cell. This modification inactivates EF-2, thereby
halting protein synthesis.
• Cell Death: The cessation of protein synthesis leads to cellular necrosis (death). In the throat, this results in tissue
damage,
inflammation, and the formation of the characteristic pseudomembrane.
▶ 5. Spread of the Toxin:
• The diphtheria toxin can spread systemically if it enters the bloodstream, affecting distant organs, including:
• Heart (Myocarditis): The toxin can damage heart muscle cells, leading to myocarditis (inflammation of the heart
muscle), which can cause heart failure and arrhythmias.
• Nerves (Neuropathy): The toxin can also affect peripheral nerves, causing neuropathy (nerve damage), leading to
weakness, paralysis, and other neurological symptoms.
• Kidneys: In severe cases, kidney damage can occur, though this is less common.
11.
VIRULENCE FACTORS OF
CORYNEBACTERIUMDIPHTHERIAE
▶ The virulence of C. diphtheriae is primarily associated with its ability to produce a potent exotoxin known as the
diphtheria toxin. Here are the main virulence factors of Corynebacterium diphtheriae:
▶ 1. Diphtheria Toxin (DT):
Toxin Is a polypeptide chain , comprises of two fragments A ( active) and B ( binding)
Fragment B binds to the host cell receptors (such as epidermal growth factor) and helps in entry of
f fragment A.
Fragment A gets internalized into the cell and then acts by the mechanism given below.
12.
• Mechanism ofdiphtheria toxin (dt)
•
Fragment A is the active fragment, which causes ADP ribosylation of elongation factor 2
(EF-2) → leads to inhibition of EF-2 → leads to inhibition of translation step of protein
synthesis
13.
• Factors regulatingtoxin production:
• The production of diphtheria toxin is dependent on various factors;
• 1) Phage coded : DT is coded by a bacteriophage called beta corynephage , carrying tox gene.
C. diphtheriae remains toxigenic as long as the phages are present inside the bacilli( lysogenic
conversion).
• 2) Iron concentration: The toxin production depends on the optimum concentration of iron (0.1
mg per litre).
:
14.
CLINICAL FEATURES OFDIPHTHERIA
▶
▶ 1. Respiratory Diphtheria (Most Common Form)
Incubation Period: The incubation period for diphtheria is typically 2 to 5 days after exposure to the
bacterium.
• Sore Throat: One of the earliest symptoms is a sore throat that can be severe and progressive.
• Fever: The patient usually develops a low-grade fever, which may become higher as the disease progresses.
• Malaise and Weakness: A general feeling of illness and fatigue often accompanies the fever.
• Swelling of the Neck: A characteristic symptom, especially in severe cases, is "bull neck" — marked swelling of the
neck due to enlarged lymph nodes and surrounding tissue inflammation.
15.
• Pseudomembrane Formation:
•A hallmark feature is the development of a grayish-white pseudomembrane on the tonsils,
pharynx, uvula, or soft palate. This membrane consists of dead cells, fibrin, and bacteria. It is
typically firmly adhered to the underlying tissues and can be difficult to remove.
• If the pseudomembrane becomes large, it can obstruct the airway, leading to difficulty breathing.
• Difficulty Breathing: As the pseudomembrane obstructs the airway, patients may experience stridor,
hoarseness, and respiratory distress.
▶ 2. Cutaneous Diphtheria
Is usually a secondary infection that follows a primary skin lesion due to trauma , allergy or
autoimmunity.
• Skin Ulcers: Diphtheria can also manifest as cutaneous diphtheria when the bacteria infect the skin. In
this form, patients develop chronic, non-healing ulcers with a grayish membrane similar to that seen in
respiratory diphtheria.
▶ 3. SystemicComplications (Toxin-mediated)
▶ The diphtheria toxin can cause severe systemic effects, especially in untreated or severe cases:
• Myocarditis: can lead to heart failure ( DCMP) and arrhythmias .
• Polyneuropathy: The diphtheria toxin can cause nerve damage, resulting in paralysis. This often begins
with the cranial nerves (e.g., facial nerve), leading to drooping eyelids, dysphagia (difficulty
swallowing), and hoarseness.
• Polyneuropathy is typically reversible in patients who survive the acute phase.
Other complications:
• Renal failure, pneumonia, encephalitis, cerebral infarction, pulmonary embolism, and serum sickness
due to antitoxin therapy.
18.
▶ 4. OTHERFORMS
• Laryngeal Diphtheria: If the infection extends to the larynx, it can cause hoarseness and difficulty
breathing, and may result in complete airway obstruction.
• Ocular Diphtheria: In rare cases, Corynebacterium diphtheriae can infect the eye, leading to conjunctivitis,
keratitis, and potentially vision loss if untreated.
19.
DIAGNOSIS OF DIPHTHERIA
▶
▶1. Clinical Diagnosis
• History and Symptoms: A detailed patient history and presentation of symptoms are important. Key
features suggestive of diphtheria include:
• Sore throat and fever
• Pseudomembrane in the throat (grayish-white, firm membrane that is difficult to remove)
• Bull neck (swelling of the neck due to enlarged lymph nodes)
• Difficulty breathing or swallowing due to airway obstruction
• Neurological signs (e.g., facial paralysis, difficulty swallowing)
20.
▶ 2. MicrobiologicalDiagnosis
Confirmation of diphtheria is usually made through microbiological cultures and molecular testing.
▶ DIRECT SMEAR MICROSCOPY:
• Specimen Collection: A throat swab is taken from the affected area (often from the pseudomembrane).
• Gram staining: Appearance: C. diphtheriae appears as gram-positive, club-shaped, and often arranged in V-
shaped or palisade arrangements (often described as “Chinese letter” pattern).
21.
ALBERT STAIN: Itis more specific for C. diphtheria , they appear as green bacilli with bluish black
metachromatic granules.
22.
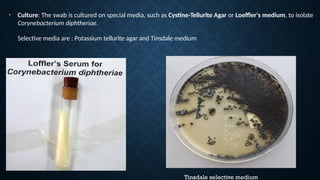
Tinsdale selective medium
•Culture: The swab is cultured on special media, such as Cystine-Tellurite Agar or Loeffler's medium, to isolate
Corynebacterium diphtheriae.
Selective media are : Potassium tellurite agar and Tinsdale medium
23.
▶ B. POLYMERASECHAIN REACTION
(PCR)
• Toxin Gene Detection: PCR can be used to detect the tox gene (which encodes the diphtheria toxin) in
Corynebacterium diphtheriae. This method is rapid and highly sensitive.
• Advantages: PCR provides a faster diagnosis compared to traditional culture methods and can
detect toxigenic strains even if the bacteria are present in low numbers.
▶ c. Elektrophoresis of Diphtheria Toxin
• Toxin Detection: by ELISA
▶ 3. Biochemical Tests
• Catalase Test: Corynebacterium diphtheriae is catalase-positive, which helps distinguish it from other
bacteria.
• Urease Test: C. diphtheria is urease negative.
24.
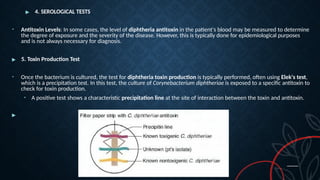
▶ 4. SEROLOGICALTESTS
• Antitoxin Levels: In some cases, the level of diphtheria antitoxin in the patient's blood may be measured to determine
the degree of exposure and the severity of the disease. However, this is typically done for epidemiological purposes
and is not always necessary for diagnosis.
▶ 5. Toxin Production Test
• Once the bacterium is cultured, the test for diphtheria toxin production is typically performed, often using Elek's test,
which is a precipitation test. In this test, the culture of Corynebacterium diphtheriae is exposed to a specific antitoxin to
check for toxin production.
• A positive test shows a characteristic precipitation line at the site of interaction between the toxin and antitoxin.
▶
25.
▶ 7. DifferentialDiagnosis
• Streptococcal pharyngitis
• Infectious mononucleosis
• Vincent’s angina (necrotizing ulcerative gingivitis)
• Candida infections in the mouth or throat
• Viral infections (e.g., Epstein-Barr virus, Herpes simplex)
▶
6. Radiological Investigations
• Chest X-ray: In cases of severe respiratory involvement, a chest X-ray may be done to assess for
airway obstruction or pneumonia, although this is not specific for diphtheria.
• Neck X-ray: In severe cases where there is swelling of the neck, a neck X-ray may show evidence of
airway narrowing or tracheal obstruction.
26.
TREATMENT OF DIPHTHERIA
▶Treatment Initiation Before Diagnosis
Due to the severity and rapid progression of diphtheria, treatment with diphtheria antitoxin should be started
immediately upon clinical suspicion, even before definitive microbiological confirmation. Early administration of
antibiotics (e.g., penicillin or erythromycin) is also critical in treating the infection and preventing the spread of
bacteria
1. Diphtheria Antitoxin (DAT)
• Purpose: The diphtheria antitoxin is used to neutralize the toxin produced by the bacteria (Corynebacterium
diphtheriae),
which is responsible for the damage to tissues such as the heart, kidneys, and nervous system.
• Administration: It is administered IV or IM as soon as the diagnosis is confirmed, even before lab results
return, because diphtheria can progress quickly.
27.
• Administration:
• Thediphtheria antitoxin ( antidiphtheric horse serum) should be administered immediately
upon suspicion of diphtheria, even before the diagnosis is confirmed.
• It is given intravenously (IV) or intramuscularly (IM), depending on the clinical severity.
• The dosage depends on the severity of the disease, which is categorized as mild, moderate, or severe.
• A test dose to be given to check for hypersensitivity
• Early stage: (<48 hrs ) : 20000 - 40000 units
• If pharyngeal membrane present : 40000 – 60000 units
• Late stage ( > 3 days, with bull neck ): 80000 – 120000 units.
▶ 2. Antibiotic Therapy:
• First-line Antibiotics:
• Penicillin G (or Penicillin V) is the drug of choice.
28.
▶ 2. AntibioticTherapy
• Erythromycin 500 MG IV QID till patient able to swallow f/b 500 mg QID ORALLY FOR 14 DAYS ( 40-
50 MG /KG/DAY)
• Procaine penicillin G 6 lakh units IM BD ( for children 12500 – 25000 u/kg IM 12 HRLY till patient
able to swallow orally then TAB PENICILLIN V 125 – 250 MG QID total for 14 days.
• These antibiotics are typically administered for 14 days.
▶ 3. Supportive Care
• Respiratory Support: Since diphtheria can cause severe airway obstruction due to the
pseudomembrane (a thick, grayish membrane in the throat), respiratory support, such as oxygen or
mechanical ventilation, may be required if breathing becomes difficult.
29.
▶ 4. Isolation
•Patients with diphtheria should be isolated to prevent the spread of infection to others. They are
typically isolated in a hospital setting until they are no longer contagious, which is usually after 48
hours of effective antibiotic therapy.
• Elimination of the organism should be documented by 2 consecutive negative cultures , after the
therapy is completed .
▶ 5. Monitoring for Complications
• Complications can include cardiac arrhythmias, nerve damage (such as peripheral
neuropathy), and kidney failure. Regular monitoring is needed to identify and
manage these potential issues promptly.
30.
▶ 7. Prevention
•Immunization: Diphtheria can be prevented with the DTaP vaccine (which combines protection against
diphtheria, tetanus, and pertussis). Vaccination is recommended for children and adults, with booster
doses given throughout life.
• A protective titre of antitoxin is : > 0.01 IU/ml .
• Adult immunization:
• Adults > 18 yrs who completed primary vaccination : Td booster dose every 10 years till 65 yrs.
• Adults > 18 yrs who have not completed primary vaccination : 3 doses are given of Td vaccine at 0 , 1 month
and 1 year.
32.
PROGNOSIS
• Mortality rate: 5 – 10 %
• May approach up to 20 % in < 5 yrs old and > 40 yrs old
• Risk factors : bullneck diphtheria, myocarditis with arrhythmias, alcoholism, Age >60
yrs and < 6 months, laryngeal tracheal and bronchial involvement .
33.
ROLE OF PROPHYLAXISIN CONTACTS
• All contacts of diphtheria patients should undergo – throat culture
• All contacts irrespective of culture results are considered for antimicrobial
prophylaxis ,TAB ERYTHROMYCIN FOR 7- 10 DAYS OR INJ BENZATHINE PENICILLIN
G 1.2 MILLION UNITS FOR CHILDREN >6YRS and 6 LAKH UNITS FOR < 6 YRS OLD.
• Contacts should receive Tdap vaccine if immunization status is unknown.
34.
DIPHTHEROIDS
• Diphtheroids orcoryneforms are the nondiphtherial corynebacteria, that usually exist as
normal commensals in the throat, skin, conjunctiva and other areas.
• However, they have been associated with invasive disease, particularly in
immunocompromised patients.
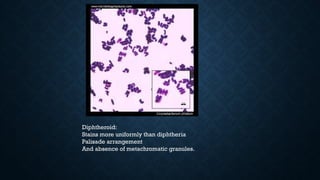
• They can be differentiated from C. diphtheriae by many features such as:
• Stains more uniformly than C. diphtheriae , Palisade arrangement: Arranged in parallel
rows rather than cuneiform pattern , Absence of metachromatic granules (except C.
xerosis).
• Coryneforms thatare rarely pathogenic to man are:
• Clinically resembling diphtheria: C. ulcerans and C. pseudotuberculosis produce
diphtheria toxin and cause localized ulcerations in throat, clinically resembling diphtheria.
• C. ulcerans causes infections in cows. Human infections may occur through cow’s milk.
• . C. pseudotuberculosis (Preisz–Nocard bacillus) causes pseudotuberculosis in sheep
and suppurative lymph- adenitis in horses. Human infection is very rare.
• C. minutissimum: It causes a localized infection of skin (axilla and groin), called as
erythrasma.’ On Wood’s lamp examination, erythrasma lesions emit coral red color
• C jeikeium:It is lipophilic species, colonizes skin of hospitalized patients. It can cause
bacteremia, endocarditis and meningitis, especially in immunocompromised hosts. It is usually
multidrug resistant, responds only to vancomycin.
• C. urealyticum: It is skin commensal, rarely causes urinary tract infection (pyelonephritis) and
alkaline encrusted cystitis (struvite stones in alkaline urine) in immunocompromised and renal
transplant recipients.
• C. pseudodiphtheriticum: It is a known commensal in throat. However in immunocompromised
patients, it can cause exudative pharyngitis (may mimic respiratory diphtheria) and endocarditis
• C. parvum is frequently used as an immunomodulator.