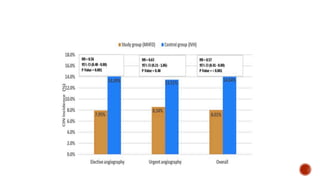
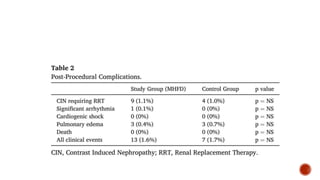
This study evaluated the benefits of a non-automated matched hydration and forced diuresis (MHFD) protocol compared to a standard hydration protocol for preventing contrast-induced nephropathy (CIN) in patients with chronic kidney disease undergoing coronary procedures. Patients received MHFD before and after the procedure, which maintained urine output above 300 ml/hour. Fewer patients developed CIN in the MHFD group compared to controls. The study suggests MHFD can effectively prevent CIN, though it was a single-center study and did not include patients with severe kidney impairment or heart failure.