INTRODUCTION
West Texas Telehealthwill provide tele monitoring and potential
future telehealth services to the aging retirement community and
patients located within the city and county limits in and around
Abilene Texas. With roughly 13% of the population being at or
above the retirement age of 65 and the ratio of clinician to patient
in Taylor county being 1 to 68 for primary care, a service such as this
may help to ease the burden of patient load that requires
monitoring services such as blood pressure, blood glucose, weight,
etc.
4.
ASSESSMENTS
ORGANIZATIONAL DESIGN
Currentcommunity need for
telehealth/telemonitoring services are not being
met
Diabetes prevalence of 10% with associated complications
Obesity prevalence of 31% with associated complications
Long waits at physician offices for routine monitoring
services of diabetes and obesity conditions
Telemonitoring service used to monitor and control glucose
levels without multiple visits
5.
ASSESSMENTS
DISPARITIES AND CULTURALCOMPETENCE
Disparities
Insurance providers may not
support telehealth/telemonitoring
Medicaid & Medicare may not
pay costs
Insurance may not recognize
patient’s home as originating
site
Federal Grant Program
Cultural Competence
Multilingual support
Monitoring services commensurate
with religious beliefs
6.
ASSESSMENTS
STRATEGIES AND ETHICALGUIDELINES
Strategies and Ethical Guidelines
Utilize current Health Information Technology (HIT)
already in place
Up to date software and hardware
ISO/TS Health Informatics, Telehealth Services
Quality Planning Guidelines
24 hours a day, 7 days a week monitoring
services
Ethical guidelines will be set by utilizing NAHQ
Code of Ethics and Standards of Practice
7.
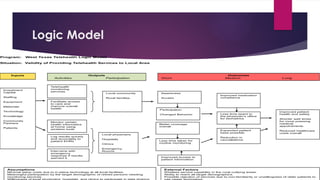
Logic Model
Program: WestTexas Telehealth Logic Model
Situation: Validity of Providing Telehealth Services to Local Area
Investment
Capital
Staffing
Equipment
Materials
Technology
Knowledge
Community
Partners
Patients
Telehealth
monitoring
services
Monitor certain
health informatics
at home using
wireless tools
Local community
Rural families
Facilitate access
to care and
improve overall
health
Local physicians
Hospitals
Clinics
Emergency
Rooms
Awareness
Access
Inputs Outputs
Activities Participation
Outcomes
Short Medium Long
Log results quickly
and accurately to
patient EHRs
Intervene with
emergency
response if results
warrant it
Expanded patient
base possible
Reduction in
cancellations
Less time taken for
routine monitoring
Better coverage
overall
Participation
Changed Behavior
Improved access to
patient information
Assumptions
Minimal setup costs due to in-place technology at all local facilities.
Meaningful participation by the target demographic of retired persons needing
monitoring services.
Willingness of local physicians, hospitals, and clinics to participate in data sharing
External Factors
Wireless service capability in the rural outlying areas.
Ability to reach all target demographics.
Possible rejection of services due to non-familiarity or unwillingness of older patients to
use newer technology.
Less time spent in
the physician’s office
for biometrics
Improved medication
compliance
Improved patient
health and safety
Shorter wait times
for more pressing
medical
appointments
Reduced healthcare
costs overall
8.
OUTCOMES
ANTICIPATED RESULTS
ShortTerm
Awareness
Access
Shortened wait time
Medium Term
Improved Compliance
Expanded patient base
Reduction in
cancellations
Long Term
Improved patient health
and safety
Shorter wait times for
more pressing medical
appointments
Reduced healthcare
costs overall
9.
OUTCOMES
EXPECTED IMPACT -COMMUNITY
Raise health awareness
Improve patient health and safety
Provide a necessary service to the area
Generate revenue sources
Improving patient, physician, and hospital
communications
10.
OUTCOMES
EXPECTED IMPACT –CULTURAL COMPLIANCE
Multilingual support added
Improving community diversity efforts and
cultural compliance
Improving health services in compliance with
various religious beliefs
Data collection to update services
11.
FINANCIAL ASPECTS
RESOURCES
ExistingHIT resources (EHRs utilized by
physician and local hospitals)
Compatible software
Wireless technology and equipment
Cell tower capability
No hard line phones or internet
connection necessary
12.
FINANCIAL ASPECTS
BUDGET ANDSUSTAINABILITY
Lack of community funds available
Federal Grant money available
Telehealth Resource Center Grant Pro
Program provides new sources of revenue
Job positions
Generate local tax monies
Possible service fee reduction from local
Telecom companies
13.
EVALUATION STRATEGY
BENCHMARKS
Costsand/or benefits gained or lost
Continual validation of service needs
Constant status of network monitored
to identify possible bottlenecks
Inclement weather impact on the
system
14.
EVALUATION STRATEGY
TOOLS USEDTO EVALUATE
Recommendations of tools from the Institute of Medicine
Race/Ethnicity/Language (R/E/L) Data
Data shows efficacy of program at reducing disparities
Stratified data shows root causes of leading disparities within
demographics
Consumer Assessment of Healthcare Providers and Systems
(CAHPS) program
Quality and Safety Review System (QSRS)
15.
CONCLUSION
With proper planning,this system should fit seamlessly into the local
healthcare community. The expected outcome would be to lower
the burden of patient load on the physicians by removing and
replacing the simple monitoring tasks with that of the telehealth
systems. The program will help to ensure healthcare equity within the
system by addressing the needs of the diverse population of the local
community and providing the necessary care and services needed to
all participating.
REFERENCES
Agency forHealthcare Research and Quality. (2016). Quality Measure Tools & Resources. Retrieved from
https://www.ahrq.gov/professionals/quality-patient-safety/quality- resources/index.html
Data USA. (2016). Taylor County Texas. Retrieved from https://datausa.io/profile/geo/taylor- county-
tx/#health
Eldercare Workforce Alliance. (2015). Caring for older adults. Retrieved from
https://eldercareworkforce.org/files/State_Issue_Briefs_2014/TX_State_Issue_Brief_-_2.14.pdf
Harrington, H. J. (2009). The Organization’s Stakeholders: Resource or Obligation? Retrieved from http://
www.qualitydigest.com/magazine/2009/may/column/organization-s-stakeholders-resource-or-
obligation.html
International Organization for Standardization. (2016, March 22). Health informatics -- Telehealth
services -- Quality planning guidelines. Retrieved from http://www.iso.org/iso/catalogue_detail?
csnumber=53052
Longest Jr., B. B. (2015). Health program management: From development through evaluation
(2nd ed.). San Francisco, CA: Jossey-Bass.
18.
REFERENCES continued
NationalAssociation for Healthcare Quality. (2016). NAHQ Code of Ethics and Standards of
Practice. Retrieved from http://www.nahq.org/Quality-
Community/content/codeethicspractice.html
National Telehealth Policy Resource Center. (2016). National Telehealth Policy Resource Center.
Retrieved from http://www.cchpca.org/national-telehealth-policy-resource-center
Robert Wood Johnson Foundation. (2014, April). Using Data to Reduce Disparities and Improve
Quality: A Guide for Health Care Organizations. Retrieved from
http://www.solvingdisparities.org/sites/default/files/data%20issue%20brief.pdf
U.S. Department of Health & Human Services. (2016). Telehealth Resource Center Grant Program.
Retrieved from https://www.hrsa.gov/ruralhealth/programopportunities/fundingopportunities/?
id=bd201808- a31c-4266-b52e-50278bd612f9
Vanderwerf, M. (2016). 10 Critical Steps for a Successful Telemedicine Program. Retrieved from
http://www.amdtelemedicine.com/downloads/10_steps.pdf
Editor's Notes
#1 Comprehensive Program Proposal Presentation
Joseph Romero
Southern New Hampshire University
IHP 670
Dr. Suzanne Paone
#2 During this presentation we will be discussing the following:
Introduction
Assessments – We will cover organizational design for program development, healthcare disparities, cultural competence, programmatic strategies and how they align with ethical guidelines.
Logic Model - Will identify the stakeholders and their relationship with the programs as well as resources, activities, inputs and outputs expected for the program.
Outcomes- All anticipated outcomes
Financial Aspects – This will cover specific resources necessary as well as budget expectations and ideas to ensure the program remains sustainable financially.
Evaluation Strategy – Evaluation methods will be discussed such as the measure methodology as well as what will be measured and what tools will be used to show incident reduction and program success.
Conclusion
#3 The agency chosen, West Texas Telehealth, will be able to provide certain telehealth services to the residents of the Abilene Texas community as well as many of the smaller surrounding outlying communities. The focus of this agency will be to cover or close the gap that exists between the number of elderly retired patients requiring some level of daily or weekly scheduled monitoring and the physicians in the area. This gap is predicted to widen by 100% in the next few years as more and more people reach the age and health level that requires more attention from physicians (Eldercare Workforce Alliance, 2015).
With roughly 13% of the population being at or above the retirement age of 65 and the ratio of clinician to patient in Taylor county being 1 to 68 for primary care (Data USA, 2016), a service such as this may help to ease the burden of patient load that requires monitoring services such as blood pressure, blood glucose, weight, etc.
#4 The servicing area, Abilene Texas and the surrounding rural areas currently have no telehealth/telemonitoring service availability unless their care is associated with the Veterans Health administration (VHA). The focus of this agency will be to cover or close the gap that exists between the number of elderly retired patients requiring some level of daily or weekly scheduled monitoring of these health problems and the physicians in the area. This gap is predicted to widen by 100% in the next few years as more and more people reach the age and health level that requires more attention from physicians (Eldercare Workforce Alliance, 2015).
Current data shows the population to be at roughly 135,000 people. Within the community, 10% of the population have diabetes and associated complications while 31% suffer from obesity with associated complications (Data USA, 2016). The areas supports a rather large retiree community as it is home to an active Air Force base. These demographic groups may be served better and faster by utilizing the monitoring services if they are linked to the above diseases and complications. This alone will greatly reduce recurring complications and alleviate long physician appointment wait times. Intervention programs may also be initiated earlier while under monitoring if the conditions worsen. This can be reinforced by the fact that long waits for local physician visits for routine medical monitoring such as blood pressure, weight management, diabetic monitoring, etc. (Vanderwerf, 2016). These monitoring tasks may be eliminated from the physician’s office through the use of a dedicated telehealth/telemonitoring program.
#5 Some disparities will undoubtedly exist when introducing a system such as this into a small retirement type community such as Abilene Texas. One such disparity may be that not every health insurance provider utilized in the area will support the use of telehealth services. Current Medicaid coverage may not cover the cost of using the system. Other payers may not even recognize the patient’s home as an originating site for the use of this service (Vanderwerf, 2016). This disparities may initially cause some delays in the implementation of services but due to the rural type setting of some of the residents, the system may qualify for federal funding through the U.S. Department of Health & Human Services Telehealth Network Grant Program (TNGP) (U.S. Department of Health & Human Services, 2016).
The establishment of the telehealth program will help to ensure healthcare equity within the system by across the diverse population of the local community by providing the necessary care and services need to all participating. This will be accomplished by providing multi-lingual support to cover all language barriers that may exist within the community. Different religions view healthcare differently and observe many different practices to stay in touch with their elected faith obligations. These beliefs will be observed and practiced by the staff whenever necessary in order to maintain religious diversity within the program.
#6 The current Health Information Technology (HIT) utilized within the local area offices and hospitals will need to be surveyed to ensure that the most reliable, up-to-date software and system hardware is being utilized in order to ensure that no immediate breakdowns will occur when the system is brought online. Of course when planning the organization, all guidance suggested in the ISO/TS Health Informatics, Telehealth Services Quality Planning Guidelines (International Organization for Standardization, 2016) will be used and adhered to in order to ensure success.
With proper planning, this system should fit seamlessly into the local healthcare community. The expected outcome would be to lower the burden of patient load on the physicians by removing and replacing the simple monitoring tasks with that of the telehealth systems. The daily/weekly results can be monitored 24 hours a day, 7 days a week by certified/trained staff that will document and notify the physicians whenever certain conditions set by the physician are met.
Where ethical guidelines are concerned, the program will utilized and adhere to the standards set forth by the National Association of Healthcare Quality in the NAHQ Code of Ethics and Standards of Practice (National Association for Healthcare Quality, 2016).
#7 Logic Model for West Texas Telehealth Program
In establishing a new tele-health service, West Texas Telehealth, organizational stakeholders will play a valuable part in ensuring the for-profit company is successful. The initial identification of organizational stakeholders for this company are investors, partners, management, employees, suppliers, local physicians/hospitals/facilities, and customers. As local physicians/hospitals/facilities and customers do have an impact on the organization, they are considered stakeholders, but internal members would be considered “organizational stakeholders (Harrington, 2009).
Investors and partners will have an important role in this endeavor as they supply the financial backing necessary to implement any and all chosen plans or paths. Next, managers and employees will be on the frontline working with the local healthcare personnel and customers to ensure that the service being provided is the best possible and that malfunctions and other problems are kept to a minimum so as to not compromise patient safety or privacy. They will be in the best position to identify any obstacles or problems early on that occur within the program as they will be in constant contact with the patients and their respective healthcare teams allowing for real-time feedback to occur.
Vendors and suppliers may also be a valuable organizational asset as they may provide updated software/hardware, training, and other telecomm services or equipment as it becomes available. They may also be able to offer maintenance services or contracts for their products that may be significantly less costly than hiring full time positions to do the same thing. Having them as stakeholders with somewhat limited input may be beneficial to both organizations as it allows this one to possibly save or reduce some costs and ensures steady business income for them as they provide these services (Harrington, 2009).
#8 Anticipated results that can be expected from establishing a telehealth/telemonitoring program can be measured in short, medium, and long term time periods (Longest Jr., 2015). In the immediate or short term time frame, an expectation of raising awareness to medical conditions, improving access to healthcare services and a shortened wait time at physician offices may be seen. Medium term outcomes may be seen in the form of improved compliance with medication or treatment plans for those suffering from things such as diabetes for example. Another benefit or outcome may be an expanded patient base as improved access and current wireless or mobile technology will aid in this endeavor. This service may also help to reduce cancellations for patients needing simple monitoring services as they will be able to do it from home. Long term improvements or outcomes would be improved patient health and safety, shorter wait times at the physician office when it is necessary to see one, and reduction of cost for healthcare services overall as quick intervention may prevent costly emergencies.
#9 Expected community outcomes will come in several different forms. Raising health awareness in the local area will surely be one of those outcomes. Helping people understand their conditions/illnesses and the best way to monitor and/or treat them will improve their over health and safety. A service such as this does not exist in this local area with the exception of those receiving healthcare from the VHA. This will also help to generate more local revenue as jobs will be created and new services will be opened up in the area to support the program. Lastly, this will impact the community through improving communication efforts between patients, physicians and local hospitals that will ultimately improve patient treatment outcomes (Vanderwerf, 2016).
#10 The establishment of the telehealth program will help to ensure healthcare equity within the system by across the diverse population of the local community by providing the necessary care and services need to all participating. This will be accomplished by providing multi-lingual support to cover all language barriers that may exist within the community. Religious beliefs or non-belief will be observed as well through cultural training and improvement programs. The collection and use of data will also be used to update and improve services that match the diversity of the clients. This will all hinge on building a foundation that supports cultural competence as part of the overall organization (Longest Jr., 2015).
#11 In order to provide a viable cost-effective and sustainable telehealth program to the local area several different resources will be necessary. The key to this viability and sustainability will be to not attempt to build the program from scratch but to integrate and utilize those valuable resources that are already in place in the community. The basic equipment requirements for the program will be secure software that will be used to access, transmit, and receive patient data and information between the patients, physicians, and facilities. Utilizing software that is compatible with software already in use in the local facilities and physicians’ offices will be the most economical approach. The next requirement will be the hardware or equipment utilized to monitor the vitals and transmit the information. Again this equipment should be compatible with the local resources and allow for expansion of measurements as the physician or healthcare team deems it necessary. The latest hardware comes equipped with the capability to utilize cell phone technology through a central service that would operate within the telehealth office. This will ensure that no internet or even phone connections are required by the client to utilize the equipment (National Telehealth Policy Resource Center, 2016).
#12 Budget concessions will be necessary as there are very few community funds for healthcare within the city. The current funding is already stretched very far and has utilized many of the state and federal grants available for the existing services. As this area is comprised of a main city population less than 150,000 and several outlying smaller towns, it fits within the government eligibility requirements for the Telehealth Resource Center Grant Program that is offered by the U.S. Department of Health & Human Services (U.S. Department of Health & Human Services, 2016). This grant funding will supplement the funding received by the investors and shareholders establishing the organization.
As this service is mostly new to this area, opportunities for new sources of revenue will be created. This will include the addition of many new job positions from staff member to technical personnel. The financial sustainability may be enhanced by seeking further partnership with the Veterans Health Administration in providing local service to their eligible clients for the telehealth program as their closest service center is over 200 miles away. Expense reductions from within the community may be had in the form of service fee reductions from local communications companies.
#13 When establishing the framework to measure the effectiveness of the program, several metrics will be necessary. There are some key areas that will be monitored within the program. Socioeconomic aspects will look at costs and benefits gained or lost within the program. Next, health domain will provide key data from each health operation within the system that is specific to the patient. Health services data will validate the need to continue, update, or discontinue services that do not benefit the program. Telehealth technologies data showing full capabilities versus bottlenecks or problem areas will be used as well. Environmental settings will also play a part in the measuring of success of the program. These will contain things such as how often local storms or weather will affect connectivity within the network (National Telehealth Policy Resource Center, 2016).
#14 Tools that will be used to measure the effect of reducing health care disparities will fall in line with that recommended by the Institute of Medicine. The most prominent is the Race/Ethnicity/Language (R/E/L) Data (Robert Wood Johnson Foundation, 2014). This data looks to identify any sub-groups within the local community that may be experiencing health care disparities based on any one of the three aforementioned criteria. This data will also help to identify if the program itself is effective in eliminating any of the existing disparities within the community. This stratified data may also be used to determine the root causes of the identified disparities allow interventions and corrections to be properly installed within the system (Robert Wood Johnson Foundation, 2014).
Other tools to be used would be the Consumer Assessment of Healthcare Providers and Systems (CAHPS) program as it utilizes patient surveys to assess their experiences with providers and service agents allowing them to identify strengths and weaknesses and make necessary corrections or adjustments in order to maintain a higher level of quality and patient safety and satisfaction throughout the year (Agency for Healthcare Research and Quality, 2016). The Quality and Safety Review System (QSRS) will use structured collected data to identify and measure any adverse events that occur within the system (Agency for Healthcare Research and Quality, 2016).
#15 With proper planning, this system should fit seamlessly into the local healthcare community. The expected outcome would be to lower the burden of patient load on the physicians by removing and replacing the simple monitoring tasks with that of the telehealth systems. The program will help to ensure healthcare equity within the system by addressing the needs of the diverse population of the local community and providing the necessary care and services needed to all participating.
#17 References
Agency for Healthcare Research and Quality. (2016). Quality Measure Tools & Resources. Retrieved from https://www.ahrq.gov/professionals/quality-patient-safety/quality-resources/index.html
Data USA. (2016). Taylor County Texas. Retrieved from https://datausa.io/profile/geo/taylor-county-tx/#health
Eldercare Workforce Alliance. (2015). Caring for older adults. Retrieved from https://eldercareworkforce.org/files/State_Issue_Briefs_2014/TX_State_Issue_Brief_-_2.14.pdf
Harrington, H. J. (2009). The Organization’s Stakeholders: Resource or Obligation? Retrieved from http://www.qualitydigest.com/magazine/2009/may/column/organization-s-stakeholders-resource-or-obligation.html
International Organization for Standardization. (2016, March 22). Health informatics --Telehealth services -- Quality planning guidelines. Retrieved from http://www.iso.org/iso/catalogue_detail?csnumber=53052
Longest Jr., B. B. (2015). Health program management: From development through evaluation (2nd ed.). San Francisco, CA: Jossey-Bass.
#18 References continued
National Association for Healthcare Quality. (2016). NAHQ Code of Ethics and Standards of Practice. Retrieved from http://www.nahq.org/Quality-Community/content/codeethicspractice.html
National Telehealth Policy Resource Center. (2016). National Telehealth Policy Resource Center. Retrieved from http://www.cchpca.org/national-telehealth-policy-resource-center
Robert Wood Johnson Foundation. (2014, April). Using Data to Reduce Disparities and Improve Quality: A Guide for Health Care Organizations. Retrieved from
http://www.solvingdisparities.org/sites/default/files/data%20issue%20brief.pdf
U.S. Department of Health & Human Services. (2016). Telehealth Resource Center Grant Program. Retrieved from https://www.hrsa.gov/ruralhealth/programopportunities/fundingopportunities/?id=bd201808- a31c-4266- b52e-50278bd612f9
Vanderwerf, M. (2016). 10 Critical Steps for a Successful Telemedicine Program. Retrieved from http://www.amdtelemedicine.com/downloads/10_steps.pdf