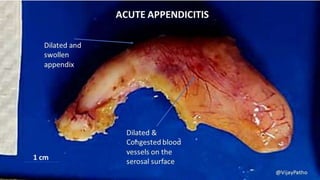
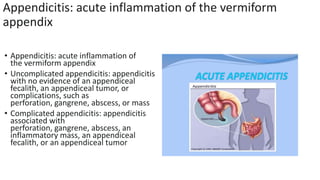
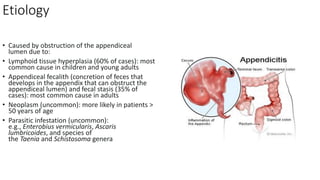
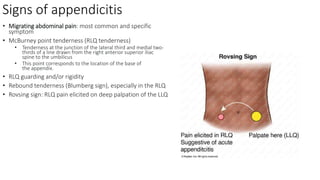
This document discusses the classification, etiology, signs and symptoms, laboratory studies, ultrasound findings, and CT imaging findings of acute appendicitis. It defines uncomplicated appendicitis as having no evidence of complications like perforation or abscess, while complicated appendicitis is associated with such complications. The most common causes are lymphoid hyperplasia in children and appendiceal fecaliths in adults, which can obstruct the appendix lumen. Key signs include migrating abdominal pain localized to the right lower quadrant, along with tenderness at McBurney's point and guarding. Laboratory tests may show a leukocytosis with elevated CRP. Ultrasound and CT imaging can detect a distended appendix

![Laboratory studies
CBC: mild leukocytosis with left
shift
• CRP: elevated (> 10 mg/L) [10]
• BMP:
↑ creatinine, electrolyte abnorm
alities may be present in patients
with
severe vomiting and diarrhea
• Urinalysis: typically normal in
appendicitis; possible findings of
mild pyuria and/or hematuria
• Urine/serum β-hCG test: perform in
all women of reproductive age to rule
out pregnancy (including ectopic
pregnancy)](https://image.slidesharecdn.com/classificationofacuteappendicitis-231212191914-8f53691a/85/Classification-of-acute-appendicitis-pptx-14-320.jpg)
![Abdominal ultrasound
• Supportive findings [10][31]
• Distended appendix (diameter > 6
mm)
• Noncompressible, aperistaltic,
distended appendix
• Target sign: concentric rings of
hypo- and hyperechogenicity in the
axial/transverse section of
the appendix](https://image.slidesharecdn.com/classificationofacuteappendicitis-231212191914-8f53691a/85/Classification-of-acute-appendicitis-pptx-15-320.jpg)
![CT abdomen with IV contrast
• CT abdomen is the most accurate
initial imaging modality for
appendicitis. [10][12][28]
• Supportive findings [28]
• Distended appendix (diameter > 6
mm)
• Edematous appendix with
periappendiceal fat stranding
• Possible appendiceal fecalith:
focal hyperdensity within the
appendiceal lumen
• Evidence of complications](https://image.slidesharecdn.com/classificationofacuteappendicitis-231212191914-8f53691a/85/Classification-of-acute-appendicitis-pptx-16-320.jpg)















































