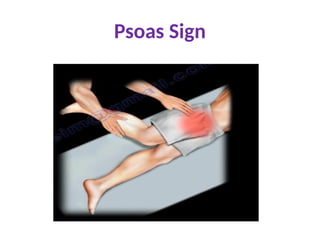
The vermiform appendix is a tubular vestigial organ attached to the caecum, commonly subject to inflammation known as acute appendicitis. Symptoms may vary depending on the anatomical position of the appendix, with common signs including peri-umbilical pain, fever, and localized tenderness at McBurney's point. Diagnosis involves imaging techniques like ultrasound and CT scans, with treatment typically involving surgical appendectomy.