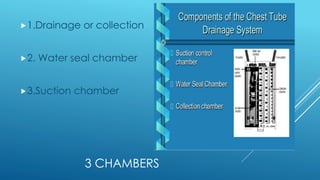
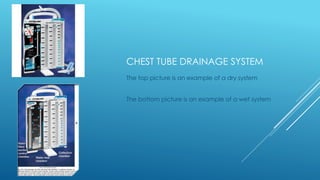
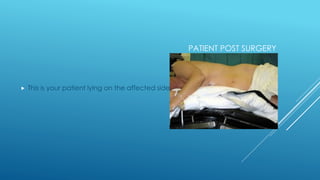
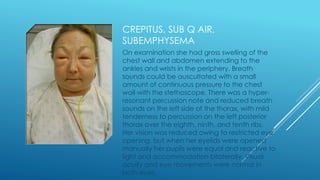
This document provides information on chest tube drainage systems. It describes the three chambers: 1) drainage collection, 2) water seal, and 3) suction. The water seal allows air to exit the chest but not re-enter. Constant bubbling in the water seal indicates an air leak, which is abnormal. Suction is applied to the third chamber to create negative pressure. Nurses must check the system every shift to ensure proper water levels, output, and that bubbling is not constant in the water seal. The document also reviews positioning of patients after surgery and important notes for nurses caring for patients with chest tubes.







































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












