Blood isa liquid connective tissue in which cells
are suspended in a fluid called plasma.
It is a viscous fluid and its specific gravity is about
1.060.
Normal pH of blood is 7.4
Total amount of blood present in the body is
about 4.5-5.5 L (70-80 mL/kg of body weight).
3.
COMPOSITION OF BLOOD
It is composed of straw colored plasma and formed elements (cells).
Composition of Plasma:
Water 93%
Electrolytes – sodium, potassium, bicarbonate, calcium, chloride etc.
Proteins- albumin, globulin, fibrinogen, etc.
Gases- oxygen, nitrogen, and CO2
Nutrients- glucose, amino acids, fatty acids, trace elements, vitamins,
lipids, cholesterol etc.
Various waste products- urea, uric acid, creatinine, bilirubin etc
Hormones- thyroxine, glucagon, insulin, etc
Enzymes- clotting factors
4.
Formed Elements(Cells) :
1. Red blood cells (RBCs)
2. White blood cells (WBCs)
3. Platelets (thrombocytes)
5.
Packed Cell Volume(PCV)
Packed Cell Volume (PCV), also known as Hematocrit,
refers to the proportion of blood volume that is occupied
by red blood cells. It is expressed as a percentage.
PCV is determined by centrifuging a blood sample,
which causes the components of blood to separate based
on their density. The red blood cells, being the heaviest,
form a layer at the bottom, while plasma remains at the
top.
The percentage of the blood volume that is made up of
red blood cells is the PCV.
Normal PCV is 40-45% of cells of blood volume, and the
remaining 55-60% of blood is plasma.
6.
The normalPacked Cell Volume (PCV) is typically between 40-45% of
the total blood volume. This means that in a given sample of blood,
40-45% of the volume consists of red blood cells (RBCs), which are
responsible for carrying oxygen throughout the body.
The remaining 55-60% of the blood is plasma, which is the liquid part
of the blood. Plasma is mostly made up of water, but it also contains
proteins (like albumin), nutrients, hormones, waste products, and
other substances that help maintain blood pressure and support
various bodily functions.
So, in simple terms:
40-45% = Red blood cells (responsible for oxygen transport).
55-60% = Plasma (the liquid part of the blood that helps in nutrient
transport and maintaining body functions).
7.
Functions of Blood
1. Transportation:
Oxygen: Blood transports oxygen from the lungs to the body's cells
and tissues via red blood cells.
Carbon Dioxide: Blood carries carbon dioxide, a waste product of
cellular metabolism, from the tissues back to the lungs for
exhalation.
Nutrients: Blood transports nutrients (e.g., glucose, amino acids,
vitamins) absorbed from the digestive system to cells throughout the
body.
Hormones: Blood carries hormones from the endocrine glands to
target organs, helping to regulate various bodily functions like
metabolism, growth, and reproduction.
Waste Products: Blood carries metabolic waste products, like urea,
to organs like the kidneys for excretion.
8.
Functions of Blood
2. Regulation:
Body Temperature: Blood helps regulate body
temperature by distributing heat throughout the body and
maintaining a stable internal temperature.
pH Balance: Blood plays a role in maintaining the acid-
base balance (pH), which is vital for normal cellular
functions. The buffer systems in blood help stabilize pH
levels.
Fluid Balance: Blood helps regulate the fluid balance
between the blood and tissues, ensuring cells have the
proper amount of water and electrolytes.
9.
Blood helpsregulate body temperature by:
Absorbing Heat: Blood absorbs heat produced by muscles
and organs.
Transporting Heat: It carries this heat through the body
via blood vessels.
Releasing Heat: Blood can release heat through the skin
by increasing blood flow to the surface, especially when
it's hot.
Conserving Heat: When it's cold, blood flow to the skin is
reduced to keep heat inside the body.
This process helps maintain a stable temperature, keeping
the body comfortable and functioning properly.
10.
Blood helpsmaintain the acid-base balance (pH) by using buffer systems
that prevent large fluctuations in pH, which are crucial for proper cell
function. Here's how it works:
Buffer Systems: These are chemical systems in the blood that resist changes
in pH. The most important buffer system in blood is the bicarbonate buffer
system.
Bicarbonate (HCO )
₃⁻ acts to neutralize excess acid (H ) by combining with
⁺
it to form carbonic acid (H CO )
₂ ₃ , which then quickly breaks down into
water (H O)
₂ and carbon dioxide (CO )
₂ .
If the blood becomes too alkaline (basic), carbonic acid can release H⁺
ions to lower the pH back to normal.
Respiratory Control: The lungs help control pH by adjusting the levels of CO₂.
When CO builds up, it reacts with water to form
₂ carbonic acid, which lowers
pH. Breathing out CO helps remove acid, raising the pH if it's too low.
₂
Kidney Control: The kidneys regulate blood pH by excreting H ions
⁺ and
reabsorbing bicarbonate (HCO )
₃⁻ . This helps balance the pH by removing
excess acids or bases.
Through these mechanisms, blood buffers and organs like the lungs and
kidneys work together to keep the pH stable, ensuring normal cellular
functions.
11.
Blood helpsregulate fluid balance between the blood and tissues by managing
the movement of water and electrolytes (such as sodium, potassium, and
chloride) between the blood vessels and surrounding tissues. Here's how it
works:
Osmotic Pressure: Blood contains proteins like albumin, which help maintain
osmotic pressure. Osmotic pressure pulls water into the bloodstream from
the surrounding tissues, preventing fluid from accumulating in the tissues
(edema).
Hydrostatic Pressure: The heart pumps blood through the blood vessels,
creating hydrostatic pressure. This pressure pushes fluid out of the blood
vessels into the tissues, providing nutrients and removing waste products.
However, the amount pushed out is balanced by the osmotic pressure, which
draws fluid back into the bloodstream.
Lymphatic System: The lymphatic system helps return any excess fluid that
leaks from blood vessels back into the bloodstream, ensuring that tissue fluid
levels remain balanced.
Kidneys: The kidneys play a key role in fluid balance by controlling how much
water and electrolytes are excreted in urine. They adjust the amount of
water reabsorbed, helping to keep the body's hydration level stable.
Through these mechanisms, blood helps ensure that cells and tissues get the
right amount of water and electrolytes to function properly, preventing
dehydration or fluid overload.
12.
Functions of Blood
3. Protection:
Immune Response: White blood cells (leukocytes) in
blood defend the body against infections, viruses,
bacteria, and other pathogens.
Clotting: Platelets and clotting factors in the blood help
prevent excessive bleeding by forming blood clots when
blood vessels are injured, promoting healing.
Antibodies: Blood contains antibodies that recognize and
neutralize foreign invaders, such as bacteria, viruses, and
toxins.
13.
Functions of Blood
4. Homeostasis:
Blood helps maintain overall homeostasis by balancing the
internal environment of the body, ensuring that various
systems work in harmony, such as regulating pressure and
fluid distribution.
These functions are vital for the overall health and
function of the body, ensuring that cells receive what they
need to operate effectively while also protecting the body
from harm.
14.
Physical characteristics ofblood
1. Color:
Bright red: Oxygen-rich blood, which is found in the
arteries, is bright red due to the oxygen binding with
hemoglobin in red blood cells.
Dark red: Oxygen-poor blood, which returns to the heart
via veins, is darker red because it has less oxygen and
more carbon dioxide.
15.
Physical characteristics ofblood
2. Viscosity:
Blood is thicker and more viscous than water due to the
presence of cells (especially red blood cells) and proteins
in the plasma. The viscosity helps blood flow through
blood vessels, but it also means that the heart has to work
harder to pump it.
The viscosity of blood can be affected by factors such as
the number of red blood cells (e.g., higher in dehydration
or polycythemia).
16.
Blood viscosityrefers to how thick or sticky the blood is.
Thicker blood flows more slowly, and the heart has to
work harder to push it through the blood vessels.
Higher Viscosity: When blood is thicker (due to more red
blood cells or higher levels of proteins), it faces more
resistance as it moves through blood vessels. This means
the heart needs to pump with more force to move the
blood.
Lower Viscosity: If the blood is thinner (for example, if it
has fewer red blood cells or less protein), it flows more
easily, and the heart doesn't have to work as hard.
So, while viscosity helps blood flow to deliver nutrients
and oxygen, a thicker blood requires more effort from the
heart to circulate efficiently.
17.
Physical characteristics ofblood
3. Volume:
The average adult has about 4.5 to 6 liters of blood,
which constitutes approximately 7-8% of body weight.
Blood volume can vary depending on factors such as age,
gender, body size, and hydration level.
18.
Physical characteristics ofblood
4. Temperature:
Blood has a temperature of about 38°C (100.4°F),
slightly higher than the normal body temperature of 37°C
(98.6°F). This helps regulate the body's overall
temperature.
19.
Physical characteristics ofblood
5. Density:
Blood has a density greater than water, usually around
1.050 to 1.060 g/mL. This is due to the solid components
(red blood cells, white blood cells, platelets) and plasma
proteins in the blood.
20.
Physical characteristics ofblood
6. pH:
Blood has a slightly alkaline pH, typically ranging from
7.38 to 7.42. This is important for maintaining proper
enzyme function and overall homeostasis. Any significant
deviation from this range can lead to health problems.
7. Specific Gravity:
The specific gravity of blood is typically around 1.050 to
1.060. This is a measure of the density of blood compared
to water.
21.
Physical characteristics ofblood
8. Composition:
Plasma: The liquid component, about 55% of blood, is
pale yellow and consists mostly of water, electrolytes,
proteins, and dissolved substances.
Formed Elements: The solid components of blood, which
include:
Red blood cells (RBCs): They are the most numerous
and give blood its color.
White blood cells (WBCs): These are fewer in number
and are involved in immune defense.
Platelets: These are small fragments involved in blood
clotting.
22.
PLASMA PROTEINS
1.Albumin:
Function: Albumin is the most abundant plasma protein,
making up about 55-60% of the total plasma protein
content.
Role:
It helps maintain osmotic pressure (also known as
oncotic pressure), which keeps fluid from leaking out of
blood vessels into tissues. This is important for
regulating blood volume and tissue fluid balance.
It acts as a carrier protein, binding and transporting
various substances such as hormones, fatty acids, and
drugs.
23.
PLASMA PROTEINS
2.Globulins:
Function: Globulins are a group of proteins that make up
around 35-40% of plasma proteins.
Types:
Alpha globulins: Involved in transporting lipids and
hormones, as well as clotting processes.
Beta globulins: Transport iron and lipids, and also play
a role in the immune system.
Gamma globulins (Immunoglobulins): These are
antibodies that play a critical role in the body's
immune response by identifying and neutralizing
foreign invaders such as bacteria, viruses, and toxins.
24.
PLASMA PROTEINS
3.Fibrinogen:
Function: Fibrinogen makes up about 4-6% of plasma
proteins and is an important protein involved in blood
clotting.
Role:
During injury, fibrinogen is converted into fibrin, which
forms a mesh-like structure to help seal wounds and
stop bleeding.
This clotting process is a vital part of wound healing
and preventing excessive blood loss.
25.
PLASMA PROTEINS
4.Prothrombin:
Function: Prothrombin is a plasma protein involved in the
blood clotting process.
Role: Prothrombin is converted to thrombin during the
clotting cascade, which is essential for fibrinogen
conversion to fibrin and the formation of a blood clot.
26.
FUNCTIONS OF PLASMAPROTEINS
Maintain Osmotic Pressure: Albumin is the primary
protein responsible for maintaining the osmotic pressure
in the blood vessels, which prevents fluid from leaking
into tissues and helps maintain blood volume.
Clotting: Fibrinogen and prothrombin are vital for blood
coagulation, preventing excessive blood loss after injury.
Immune Response: Globulins, especially gamma globulins
(immunoglobulins), are antibodies that defend the body
against infections.
Transport: Plasma proteins transport various molecules,
including hormones, nutrients, waste products, and gases,
throughout the body.
27.
Normal Total PlasmaProtein Level
Total proteins: 6.4 to 8.3 g/dL (grams per deciliter) for
adults.
Albumin: 3.5 to 5 g/dL
Globulin: 1.5 to 2.5 g/dL
Fibrinogen: 150 to 300 mg/dL
28.
FORMATION OF BLOODCELLS
The formation of blood cells, known as hematopoiesis, is a
complex process in which blood cells are produced from stem
cells in the bone marrow.
Hematopoiesis ensures that the body maintains a steady supply
of red blood cells, white blood cells, and platelets, all of which
have essential roles in the body's function and defense.
Sites of Hematopoiesis:
Fetal Development: During early fetal development,
hematopoiesis occurs in various sites, including the yolk sac,
liver, and spleen.
After Birth: In adults, hematopoiesis mainly occurs in the bone
marrow (particularly in flat bones like the sternum, ribs,
pelvis, and skull).
29.
Hematopoiesis Process
Hematopoiesisoccurs through the differentiation
and maturation of hematopoietic stem cells
(HSCs), which are multipotent cells capable of
giving rise to all types of blood cells. This process
is regulated by growth factors and cytokines.
30.
Process ofHematopoiesis:
Stem Cells: The process starts with hematopoietic stem cells
(HSCs) in the bone marrow, which are multipotent (can
become many types of cells).
Differentiation: These stem cells differentiate into specialized
precursor cells for each type of blood cell.
Maturation: These precursor cells mature into fully functional
blood cells, which then enter the bloodstream to perform their
respective functions.
Major Stages of Hematopoiesis:
Erythropoiesis: Formation of red blood cells.
Leukopoiesis: Formation of white blood cells.
Thrombopoiesis: Formation of platelets.
31.
Stages of BloodCell Formation
1. Hematopoietic Stem Cells (HSCs):These stem cells are
pluripotent, meaning they can develop into any type of blood cell.
HSCs reside in the bone marrow and are capable of self-renewal,
ensuring a constant supply of blood cells throughout life.
2. Common Myeloid Progenitor (CMP) and Common Lymphoid
Progenitor (CLP):
Hematopoietic stem cells differentiate into two main progenitor
cells:
CMP (Common Myeloid Progenitor): Gives rise to red blood cells,
platelets, and most white blood cells (except lymphocytes).
CLP (Common Lymphoid Progenitor): Differentiates into
lymphocytes (T cells, B cells, natural killer cells).
32.
Progenitor cellsand precursor cells are both types of cells
involved in the development of blood cells, but they have
distinct roles:
Progenitor cells: These are early, partially differentiated
cells that can still divide and form different types of blood
cells, but they have a more limited potential than stem
cells. They are more specific in what types of blood cells
they can become.
Precursor cells: These are more mature than progenitor
cells. They are committed to becoming a specific type of
blood cell and undergo further development and
differentiation until they become fully mature blood cells.
In short, progenitor cells are more versatile than precursor
cells, but precursor cells are closer to becoming fully
functional blood cells.
33.
Stages of BloodCell Formation
3. Lineages of Blood Cells:
From the CMP and CLP, various specialized cells develop in distinct
lineages:
Erythropoiesis (Formation of Red Blood Cells):
Proerythroblast → Erythroblast → Normoblast → Reticulocyte →
Mature Red Blood Cell (Erythrocyte)
Red blood cells (RBCs) are responsible for oxygen transport. The
key regulation factor for RBC production is erythropoietin (EPO),
a hormone produced by the kidneys in response to low oxygen
levels.
34.
Stages of BloodCell Formation
Leukopoiesis (Formation of White Blood Cells):
White blood cells (WBCs) are formed from the myeloid lineage
(granulocytes and monocytes) and the lymphoid lineage
(lymphocytes).
Granulocytes (e.g., neutrophils, eosinophils, basophils):
Myeloblast → Promyelocyte → Myelocyte → Metamyelocyte
→ Mature Granulocyte
Monocytes (precursors of macrophages):
Monoblast → Promonocyte → Monocyte
Lymphocytes (T cells, B cells, NK cells):
Lymphoid progenitor → Immature lymphocyte → Mature
lymphocyte (T or B cells)
35.
Stages of BloodCell Formation
Thrombopoiesis (Formation of Platelets):
Platelets are produced from megakaryocytes in the bone marrow.
Megakaryoblast → Megakaryocyte Platelets (small cell
→
fragments)
The production of platelets is regulated by thrombopoietin, a
hormone mainly produced by the liver and kidneys.
36.
Regulation of Hematopoiesis
Hematopoiesis is controlled by a complex network of
growth factors and cytokines that influence the
differentiation and maturation of blood cells:
1. Erythropoietin (EPO): Stimulates the production of red
blood cells in response to low oxygen levels.
2. Granulocyte colony-stimulating factor (G-CSF): Stimulates
the production of neutrophils.
3. Thrombopoietin (TPO): Regulates the production of
platelets.
4. Interleukins: A group of cytokines that play key roles in
the development of various white blood cells.
37.
Interleukins andcytokines are both types of signaling molecules that
help regulate immune responses and the development of blood cells,
but they have some differences:
Cytokines: These are a broad group of proteins, peptides, or
glycoproteins that act as signals between cells. They play a role in
immune responses, inflammation, and the development of blood
cells. Cytokines include interleukins, interferons, growth factors, and
other signaling molecules.
Interleukins: These are a specific type of cytokine. They are
primarily involved in communication between white blood cells
(leukocytes) and play a key role in regulating immune responses,
inflammation, and hematopoiesis (the production of blood cells).
In short, all interleukins are cytokines, but not all cytokines are
interleukins.
38.
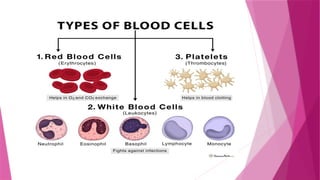
Types of BloodCells Formed
1. Red Blood Cells (Erythrocytes): Carry oxygen from the
lungs to tissues and return carbon dioxide to the lungs.
2. White Blood Cells (Leukocytes): Part of the immune
system; they protect the body against infections and
foreign invaders.
Granulocytes: Neutrophils, eosinophils, basophils.
Agranulocytes: Lymphocytes (T cells, B cells, NK cells),
monocytes.
3. Platelets (Thrombocytes): Involved in blood clotting to
prevent excessive bleeding.
39.
RED BLOOD CELLS(ERYTHROCYTES)
These cells are a crucial component of the blood and have the
primary function of transporting oxygen from the lungs to the
rest of the body and carrying carbon dioxide back to the lungs
to be exhaled.
Erythrocytes are unique because they:
1. Lack a nucleus: This allows them to carry more hemoglobin,
the protein responsible for binding oxygen.
2. Are biconcave in shape: This shape increases their surface
area for gas exchange and helps them squeeze through narrow
capillaries.
3. Contain hemoglobin: This iron-rich protein binds to oxygen
molecules, allowing RBCs to carry oxygen.
Erythrocytes are produced in the bone marrow and typically
have a lifespan of about 120 days.
40.
HAEMOGLOBIN
Hemoglobin isa protein found in erythrocytes (red blood
cells) that plays a crucial role in oxygen transport. It is
responsible for binding oxygen in the lungs and releasing it
in tissues throughout the body.
The structure of hemoglobin is complex and essential for
its function in oxygen transport. It is a quaternary
protein, meaning it consists of multiple protein subunits
that work together.
41.
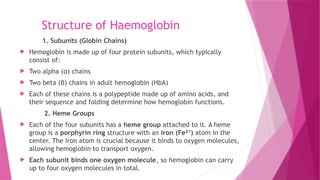
Structure of Haemoglobin
1.Subunits (Globin Chains)
Hemoglobin is made up of four protein subunits, which typically
consist of:
Two alpha (α) chains
Two beta (β) chains in adult hemoglobin (HbA)
Each of these chains is a polypeptide made up of amino acids, and
their sequence and folding determine how hemoglobin functions.
2. Heme Groups
Each of the four subunits has a heme group attached to it. A heme
group is a porphyrin ring structure with an iron (Fe² )
⁺ atom in the
center. The iron atom is crucial because it binds to oxygen molecules,
allowing hemoglobin to transport oxygen.
Each subunit binds one oxygen molecule, so hemoglobin can carry
up to four oxygen molecules in total.
42.
Haemoglobin Variants
AdultHaemoglobin (HbA): The typical adult form, with
two alpha and two beta chains.
Foetal Haemoglobin (HbF): Foetal haemoglobin has two
alpha and two gamma chains, which have a higher affinity
for oxygen than adult haemoglobin. This allows foetuses to
extract oxygen from the mother’s blood more efficiently.
Haemoglobin S (HbS): In sickle cell disease, haemoglobin
undergoes a mutation in the beta chains, causing them to
polymerize under low oxygen conditions, leading to the
sickling of red blood cells.
43.
Normal values ofhaemoglobin
The normal values of hemoglobin can vary depending on
factors like age, sex, and sometimes altitude.
1. Adults:
Men: 13.8 to 17.2 grams per deciliter (g/dL)
Women: 12.1 to 15.1 grams per deciliter (g/dL)
2. Children:
Newborns: 14 to 24 g/dL (higher at birth but decreases
after the first few months)
Infants (6 months to 1 year): 10.5 to 13.5 g/dL
Children (1 to 12 years): 11.5 to 15.5 g/dL
44.
Normal values ofhaemoglobin
3. Pregnancy:
Pregnant Women: Hemoglobin levels may be slightly
lower during pregnancy due to an increase in plasma
volume. A common range is 11 to 15 g/dL.
4. Altitude Considerations:
People living at higher altitudes may have slightly higher
hemoglobin levels due to the lower oxygen availability,
which stimulates the body to produce more red blood
cells.
45.
Functions of RBCs
Transporting oxygen to tissues and organs. This is
accomplished via hemoglobin, a protein in RBCs that
binds to oxygen in the lungs and releases it in tissues
where it is needed for energy production.
Removing carbon dioxide from tissues and carrying it to
the lungs.
Facilitating smooth blood flow and maintaining circulatory
system health. RBCs contribute to blood viscosity, which
affects how easily blood flows through the circulatory
system. The shape of RBCs (biconcave disc shape) allows
them to move smoothly through small capillaries, which is
vital for efficient gas exchange in tissues.
46.
Additional Functions
Whilethe main roles of RBCs are oxygen transport and
carbon dioxide removal, their other supportive functions
are essential for overall circulatory and respiratory health:
Flexibility and Deformability: RBCs are very flexible,
which allows them to squeeze through narrow capillaries
(as small as 2-3 microns in diameter) without breaking.
Their biconcave shape increases surface area for better
gas exchange.
Lifespan and Recycling: RBCs have a lifespan of about 120
days. After their life cycle, they are removed from
circulation and broken down by the spleen and liver. The
iron from the hemoglobin is recycled and used to produce
new RBCs in the bone marrow.
47.
Erythropoiesis
Erythropoiesis isthe process by which red blood cells (RBCs) are
produced. This process takes place primarily in the bone marrow
and involves the differentiation and maturation of precursor
cells into functional erythrocytes (RBCs). Erythropoiesis is tightly
regulated by the hormone erythropoietin (EPO), which
stimulates the production of RBCs in response to low oxygen
levels in the blood.
The production of RBCs is regulated by a feedback mechanism
that is largely controlled by erythropoietin (EPO), a hormone
produced primarily by the kidneys. When oxygen levels in the
blood are low (hypoxia), the kidneys detect this and release
more erythropoietin into the bloodstream. EPO stimulates the
bone marrow to increase the production of RBCs.
48.
The feedback systemcontrolled by erythropoietin (EPO)
works to maintain proper oxygen levels in the blood. Here's
how it works:
Low oxygen levels (hypoxia) in the blood are detected by
the kidneys.
In response, the kidneys release more erythropoietin
(EPO) into the bloodstream.
EPO stimulates the bone marrow to produce more red
blood cells (RBCs).
As the number of RBCs increases, oxygen levels in the
blood rise.
When oxygen levels return to normal, the production of
EPO slows down, maintaining balance.
This feedback system helps ensure that the body produces
the right amount of RBCs to meet oxygen needs.
49.
Key Stages ofErythropoiesis
1. Hematopoietic Stem Cell (HSC): Multipotent stem cells in
the bone marrow capable of differentiating into RBCs and
other blood cells.
2. Proerythroblast: The first committed precursor to RBCs
that starts the process of RBC formation.
3. Basophilic Erythroblast: Immature RBCs with high RNA
content, which is used to produce hemoglobin.
4. Polychromatic Erythroblast: The cell starts accumulating
more hemoglobin, with a color shift towards red due to
the increased hemoglobin content.
50.
5. Orthochromatic Erythroblast(Normoblast): The last stage
before nucleus ejection; these cells are highly
hemoglobinized.
6. Reticulocyte: Nucleus is ejected, and the cell enters the
bloodstream. It still contains some residual organelles like
RNA.
7. Mature Erythrocyte (RBC): After 1-2 days in circulation,
reticulocytes mature into functional RBCs, which last around
120 days.
8. Senescence and Removal: After 120 days, aged RBCs are
broken down by macrophages in the spleen and liver, and
components like iron are recycled.
51.
Importance of Erythropoiesis
Erythropoiesis ensures the continuous supply of RBCs,
which are essential for delivering oxygen to tissues and
organs and removing carbon dioxide.
The process is tightly regulated to maintain a balance in
the number of RBCs in circulation. Too few RBCs can lead
to anemia, while too many can lead to polycythemia.
52.
WHITE BLOOD CELLS
White Blood Cells (WBCs), also known as leukocytes, are
a crucial part of the immune system. They help the body
fight infections and other diseases by identifying and
attacking harmful pathogens like bacteria, viruses, and
parasites. WBCs are produced in the bone marrow and are
found in the bloodstream, lymphatic system, and tissues.
53.
There arefive main types of white blood cells, each with a distinct
function in immune response. These types can be divided into two
categories: granulocytes and agranulocytes.
1. Granulocytes:
Granulocytes have granules in their cytoplasm and play an essential
role in immune defense, particularly in fighting infections. They are
the most abundant WBCs and are subdivided into three types:
Neutrophils (60-70% of total WBC count)
Function: Neutrophils are the first responders to infection. They
are particularly effective at phagocytosis, which involves
engulfing and digesting bacteria and other pathogens.
Appearance: These cells have a multi-lobed nucleus and granules
that contain enzymes to fight infections.
54.
Eosinophils (1-4%of total WBC count)
Function: Eosinophils are involved in defending the body against
parasites (such as worms) and play a role in allergic reactions
(like asthma and hay fever).
Appearance: Eosinophils have a bilobed nucleus and large, red-
staining granules that contain toxic proteins for fighting parasites.
Basophils (0.5-1% of total WBC count)
Function: Basophils release histamine during allergic reactions
and inflammation. Histamine causes blood vessels to dilate,
increasing blood flow to the affected area.
Appearance: Basophils have a large, irregular nucleus and dark
blue-staining granules, which contain histamine and heparin (an
anticoagulant).
55.
2. Agranulocytes:
Agranulocytesdo not have visible granules in their cytoplasm and
include the following two types:
Lymphocytes (20-30% of total WBC count)
Function: Lymphocytes are crucial for the adaptive immune
response and are involved in recognizing and responding to
specific pathogens.
Subtypes:
T lymphocytes (T cells): Help control immune responses,
destroy infected cells, and regulate the immune system.
B lymphocytes (B cells): Produce antibodies that target and
neutralize pathogens.
Natural Killer (NK) cells: Play a role in identifying and killing
tumor cells or infected cells.
Appearance: Lymphocytes are round cells with a large, spherical
nucleus and a thin rim of cytoplasm.
56.
Monocytes (2-8%of total WBC count)
Function: Monocytes are the largest type of WBC. They
mature into macrophages when they enter tissues.
Macrophages are responsible for phagocytosis of
pathogens and dead cells. They also play a role in
stimulating other immune cells.
Appearance: Monocytes have a large, kidney-shaped or
oval nucleus, and their cytoplasm is abundant and pale.
58.
Normal White BloodCell Count (WBC Count)
The normal range for total WBC count in adults is
approximately:
4,000 to 11,000 WBCs per microliter of blood
(cells/µL)
The count can vary based on several factors, including
age, gender, and health condition.
59.
Differential WBC Count
Adifferential WBC count measures the percentage of each
type of white blood cell in the total count. This can help
doctors assess the cause of an infection or other health
condition. The general normal distribution for each type of
WBC is as follows:
Neutrophils: 60-70%
Lymphocytes: 20-30%
Monocytes: 2-8%
Eosinophils: 1-4%
Basophils: 0.5-1%
60.
Functions of WhiteBlood Cells (WBCs)
Immunity: WBCs are crucial in protecting the body against
pathogens. They identify, attack, and destroy harmful
agents like bacteria, viruses, fungi, and parasites.
Inflammation Response: WBCs are involved in the
inflammatory process, which helps the body fight
infections and repair tissue damage. When there is an
infection or injury, WBCs migrate to the site of infection
to help fight the invading pathogens.
Phagocytosis: Certain WBCs, such as neutrophils and
monocytes/macrophages, are able to engulf and digest
pathogens, dead cells, and debris through a process called
phagocytosis.
61.
Functions of WhiteBlood Cells (WBCs)
Antibody Production: B lymphocytes produce antibodies
(immunoglobulins), which bind to pathogens and mark
them for destruction by other immune cells.
Immune Regulation: T lymphocytes help regulate immune
responses by activating or suppressing other immune cells,
ensuring that the immune system responds appropriately
to threats without attacking the body’s own cells.
62.
Abnormal WBC Counts
Leukocytosis: An increase in the number of WBCs above
the normal range, often indicating an infection,
inflammation, or leukemia. Increase in total WBC count
above 11,000/mm³
Leukopenia: A decrease in the number of WBCs, which
can make the body more susceptible to infections. Causes
of leukopenia include bone marrow disorders,
autoimmune diseases, and certain medications.
Decrease in count below 4000/mm³
63.
Factors Influencing WBCCount
Infections: Viral or bacterial infections often result in an
increase in specific types of WBCs (e.g., neutrophils for
bacterial infections).
Medications: Some medications, especially steroids, can
cause an increase in WBC count, while chemotherapy or
immunosuppressive drugs can reduce the WBC count.
Stress: Physical or emotional stress can lead to an
increase in WBCs due to the body’s response to stress.
Allergies: Conditions like asthma or allergic reactions may
result in increased eosinophil count.
64.
PLATELETS
Platelets areoval discs, 2- 4 micrometres in diameter.
Platelets are formed from megakaryocytes, which are
largest cells of bone marrow.
Platelets are mainly involved in HEMOSTASIS (prevention
of blood loss).
65.
PLATELETS
Platelets aresmall, colorless cell fragments in the blood
that are crucial for blood clotting (hemostasis). They are
produced in the bone marrow and help stop bleeding by
clumping and forming plugs in blood vessel injuries.
Platelet Count: A normal platelet count in the blood is
typically between 150,000 and 450,000 platelets per
microliter of blood. Low platelet count
(thrombocytopenia) can cause easy bruising or excessive
bleeding, while a high platelet count (thrombocytosis) can
lead to clotting issues.
Lifespan: Platelets have a relatively short lifespan of
about 7-10 days, after which they are removed by the
spleen.
66.
FUNCTIONS
Blood clotting:Platelets stick to the site of a blood vessel
injury and each other to form a temporary plug, which
helps prevent further blood loss.
Activation: When a blood vessel is injured, platelets
become activated. They change shape, become sticky, and
release substances that attract even more platelets to the
injury site.
Coagulation: Platelets help in the activation of clotting
factors that form a more stable clot, eventually leading to
the sealing of the injury.
Platelets are essential for wound healing and preventing
excessive blood loss, making them vital components of the
circulatory system.
67.
THROMBOPOIESIS
Thrombopoiesis isthe process by which platelets
(thrombocytes) are produced in the body. It occurs in the
bone marrow and involves the development and
maturation of megakaryocytes, the large cells responsible
for platelet formation. Here's a breakdown of the process:
1. Stem Cell Differentiation
Thrombopoiesis begins with hematopoietic stem cells
(HSCs) in the bone marrow. These stem cells give rise to
all blood cells, including platelets.
The HSCs differentiate into megakaryocyte progenitors,
which eventually mature into megakaryocytes.
68.
2. Megakaryocyte Development
Megakaryocyte progenitor cells undergo endomitosis, a
process where the cell's DNA replicates without cell
division. This results in a polyploid megakaryocyte (a cell
with multiple sets of chromosomes).
As the megakaryocyte matures, it grows significantly in
size and becomes multinucleated.
3. Platelet Formation
The megakaryocyte’s cytoplasm extends into long,
branching structures called proplatelets, which resemble
arms or tentacles.
These proplatelets eventually break off into smaller
fragments, which are the platelets. Each megakaryocyte
can release thousands of platelets into the bloodstream.
69.
4. Regulation byThrombopoietin
The key regulator of thrombopoiesis is thrombopoietin
(TPO), a hormone primarily produced in the liver and
kidneys.
TPO stimulates the production and maturation of
megakaryocytes, and it also plays a role in platelet
production.
Thrombopoietin binds to receptors on megakaryocytes and
their precursors, encouraging their growth and maturation
into functional megakaryocytes.
5. Platelet Release into Bloodstream
Once formed, platelets enter the bloodstream through the
sinusoidal capillaries in the bone marrow. From there,
they circulate throughout the body, ready to respond to
injury.
70.
Lifespan of Platelets
Platelets are short-lived, typically lasting around 7–10
days in circulation. After that, they are removed by
macrophages in the spleen and liver.
71.
Disorders Related toThrombopoiesis
1. Thrombocytopenia: A low platelet count, which can
result from issues in thrombopoiesis or excessive platelet
destruction.
2. Thrombocytosis: An abnormally high platelet count,
which can increase the risk of blood clotting disorders.
3. Megakaryocytic Dysplasia: Abnormalities in the
development of megakaryocytes, which can lead to
platelet production issues.
Thrombopoiesis is crucial for maintaining a healthy
platelet count, ensuring proper blood clotting, and
facilitating wound healing.
72.
CLOTTING FACTORS
Clottingfactors are proteins in the blood that work
together to form a blood clot. The process of clot
formation, called coagulation, is essential for stopping
bleeding after injury. These factors are typically named
using Roman numerals (I, II, III, IV, etc.) and are often
referred to as the "coagulation cascade.“
1. Factor I (Fibrinogen):
Role: Fibrinogen is a soluble protein that is converted into
fibrin by the enzyme thrombin during clotting.
Function: Fibrin forms a mesh that traps blood cells and
platelets, creating the structure of a clot.
73.
2. Factor II(Prothrombin):
Role: Prothrombin is a precursor protein that is converted
into thrombin.
Function: Thrombin is a key enzyme that converts
fibrinogen into fibrin and also activates other clotting
factors in the cascade.
3. Factor III (Tissue Factor or Thromboplastin):
Role: Tissue factor is a membrane-bound protein present
on cells outside the blood vessels, typically in tissue or
damaged endothelial cells.
Function: It activates Factor VII and plays a crucial role in
the extrinsic pathway of coagulation. It interacts with
Factor VII to initiate the clotting cascade.
74.
4. Factor IV(Calcium ions, Ca² ):
⁺
Role: Calcium ions are essential for various steps in the
coagulation process.
Function: Calcium ions (Ca² ) are required for the
⁺
activation of several clotting factors and for the proper
function of the coagulation cascade.
5. Factor V (Proaccelerin or Labile Factor):
Role: Factor V is a cofactor for Factor Xa in the
conversion of prothrombin to thrombin.
Function: It helps accelerate the process of thrombin
generation, playing a key role in the common pathway of
coagulation.
75.
6. Factor VII(Proconvertin or Stable Factor):
Role: Factor VII is activated by tissue factor (Factor III) in
the extrinsic pathway of coagulation.
Function: Activated Factor VII (VIIa) activates Factor X,
which is crucial for the conversion of prothrombin into
thrombin.
7. Factor VIII (Anti-hemophilic Factor):
Role: Factor VIII is a cofactor for Factor IX in the intrinsic
pathway of coagulation.
Function: It helps activate Factor X, which is required to
produce thrombin and ultimately fibrin.
76.
8. Factor IX(Christmas Factor):
Role: Factor IX is activated by Factor XIa in the intrinsic
pathway.
Function: Activated Factor IX (IXa), with the help of
Factor VIII, activates Factor X to initiate the common
pathway.
9. Factor X (Stuart-Prower Factor):
Role: Factor X is activated by either Factor VIIa (in the
extrinsic pathway) or Factor IXa (in the intrinsic pathway).
Function: Activated Factor X (Xa) converts prothrombin
into thrombin, leading to the formation of fibrin.
77.
10. Factor XI(Plasma Thromboplastin Antecedent):
Role: Factor XI is activated by Factor XIIa in the intrinsic
pathway.
Function: Activated Factor XIa activates Factor IX, which
plays a role in the activation of Factor X.
11. Factor XII (Hageman Factor):
Role: Factor XII is activated upon contact with negatively
charged surfaces (e.g., collagen exposed in injured blood
vessels).
Function: Activated Factor XIIa activates Factor XI, and
also plays a role in the intrinsic pathway, although its
direct role in clotting is less critical than other factors.
78.
12. Factor XIII(Fibrin-stabilizing Factor):
Role: Factor XIII is activated by thrombin.
Function: Activated Factor XIIIa cross-links fibrin strands
to stabilize the fibrin clot and make it more durable.
Clotting Cascade Overview:
Extrinsic Pathway: Initiated by the exposure of tissue
factor (Factor III) due to vessel injury. Tissue factor
interacts with Factor VII to activate Factor X, leading to
thrombin generation.
Intrinsic Pathway: Involves the activation of Factors XII,
XI, IX, and VIII, culminating in the activation of Factor X.
Common Pathway: Both the intrinsic and extrinsic
pathways converge at Factor X, which is activated to Xa,
converting prothrombin into thrombin. Thrombin then
converts fibrinogen into fibrin, leading to clot formation.
79.
Key Points:
Fibrin (I) is the final product that creates the clot mesh.
Thrombin (II) plays a central role by activating other
factors and converting fibrinogen to fibrin.
Calcium (IV) is essential for nearly all steps in the clotting
cascade.
Factor VIII and Factor IX are often associated with
hemophilia, a bleeding disorder.
80.
Clotting mechanism ofblood
The clotting mechanism of blood, also known as
hemostasis, is the process by which blood forms clots to
prevent excessive bleeding when blood vessels are
injured. It involves a series of steps to stop bleeding and
repair blood vessel damage.
1. Vascular Spasm (Vasoconstriction)
When a blood vessel is injured, the smooth muscle in the
vessel wall contracts (vasoconstriction) to reduce blood
flow. This is an immediate response to limit blood loss and
is usually temporary.
81.
2. Platelet PlugFormation
Platelet Adhesion: Platelets (small cell fragments in the
blood) are attracted to the site of injury, where the
exposed collagen fibers in the damaged vessel wall are
exposed.
Platelet Activation: Upon contact with collagen, platelets
become activated and release various substances, such as
ADP, serotonin, and thromboxane A2, which attract more
platelets to the site.
Platelet Aggregation: The activated platelets stick to
each other (aggregation) and form a temporary "platelet
plug" that helps cover the breach in the vessel wall.
82.
3. Coagulation (BloodClotting)
The clotting process involves a series of chemical
reactions that activate clotting factors (proteins)
in the blood. These factors are usually present in
an inactive form, but they become activated in a
sequence called the coagulation cascade.
The coagulation cascade is divided into three
stages:
83.
a) Intrinsic Pathway:
This pathway is triggered when blood comes into contact
with damaged tissue. It involves several clotting factors
(such as factor XII, XI, IX, and VIII) that are activated in a
chain reaction, eventually leading to the activation of
factor X.
b) Extrinsic Pathway:
This pathway is triggered by tissue factor (TF), which is
released from the damaged vessel. TF combines with
factor VII, which activates factor X.
84.
c) Common Pathway:
Both the intrinsic and extrinsic pathways converge at the
activation of Factor X, which plays a central role in blood
clotting.
Activated Factor X (Xa) combines with Factor V, calcium
ions (Ca² ), and phospholipids to form
⁺ prothrombinase.
This complex converts prothrombin into thrombin.
Thrombin then converts fibrinogen (a soluble plasma
protein) into fibrin, which forms a mesh-like structure
that traps blood cells and strengthens the clot.
85.
4. Clot Retractionand Repair
After the clot forms, it contracts (clot retraction) to
reduce the size of the wound and help close the blood
vessel.
Tissue repair begins shortly after clot formation, with the
help of growth factors released by platelets. This process,
called fibrinolysis, eventually removes the clot once the
vessel has healed.
86.
5. Fibrinolysis (ClotRemoval)
After the blood vessel has healed, the clot is no longer
needed. Plasminogen, which is incorporated into the clot,
is activated to plasmin. Plasmin breaks down fibrin and
dissolves the clot.
87.
Summary:
The bloodclotting mechanism involves:
Vascular spasm to limit blood flow.
Platelet plug formation to provide temporary coverage.
Coagulation (involving intrinsic, extrinsic, and common
pathways) to form a stable fibrin clot.
Clot retraction and repair to close the wound.
Fibrinolysis to remove the clot once healing is complete.
This coordinated series of events ensures that bleeding is
minimized and that the blood vessel can repair itself.
88.
BLEEDING TIME &CLOTTING TIME
It is the time interval between the start of bleed and its
arrest.
Normal bleeding time is 1 to 6 minutes.
Bleeding time can be prolonged with a decrease in the
platelet count.
Clotting time: it is the time interval between oozing of
blood and clot formation. It is 3 – 9 minutes.
89.
BLOOD GROUPS
Onthe surface of RBC of a person, blood group antigens
are present that are termed as agglutinogens.
The most important blood group systems are ABO system
and Rh.
Blood groups refer to the classification of blood based on
the presence or absence of specific antigens on the
surface of red blood cells.
90.
ABO Blood GroupSystem
The ABO system classifies blood into four main groups: A,
B, AB, and O.
These groups are determined by the presence or absence
of two antigens: A and B.
Group A: Has antigen A.
Group B: Has antigen B.
Group AB: Has both antigen A and antigen B.
Group O: Has neither antigen.
91.
Each agglutinogenis capable of combining with a specific
antibody called agglutinin present in plasma.
If a particular agglutinogen is absent in a persons RBCs,
the corresponding agglutinin is present in plasma.
Therefore, A group people have anti-B or beta agglutinins.
B group people have anti-A or alpha agglutinins.
AB group people donot have agglutinins.
O group people contain both alpha and beta agglutinins in
the plasma.
92.
Landsteiner's Law
Landsteiner'sLaw is a principle that governs the
inheritance and compatibility of blood groups. It is named
after the Austrian immunologist Karl Landsteiner, who
discovered the ABO blood group system and made
significant contributions to immunology.
This law plays a critical role in understanding blood
transfusions and compatibility, as it helps explain why
receiving blood from the wrong type can cause an immune
response.
93.
Landsteiner's Lawstates that a person will produce
antibodies against the antigens they do not have on
their red blood cells. In other words:
If a person has blood group A, their immune system will
produce anti-B antibodies, because they don't have
antigen B on their red blood cells.
If a person has blood group B, they will produce anti-A
antibodies, because they don't have antigen A.
If a person has blood group AB, they will not produce any
anti-A or anti-B antibodies because they have both
antigens on their red blood cells.
If a person has blood group O, they will produce anti-A
and anti-B antibodies, because they have neither antigen
A nor antigen B.
94.
Why is itimportant?
Blood Transfusions: Understanding Landsteiner's Law is
crucial when performing blood transfusions. If
incompatible blood is transfused, the antibodies present
in the recipient's blood will attack the foreign blood cells,
leading to serious reactions.
Organ Transplants: It is important to match both ABO and
Rh groups when considering organ donations to prevent
rejection of the organ.
95.
Determination of bloodgroup
The determination of a blood group involves testing the
presence or absence of specific antigens on the surface of
red blood cells and identifying the antibodies present in
the plasma.
Steps for Determining Blood Group:
1. Collecting a Blood Sample
A small sample of blood is usually collected from the
individual using a syringe or fingerstick.
2. ABO Blood Group Test
Reagents: The test uses anti-A and anti-B sera (reagents).
These are solutions containing antibodies that will react
specifically with the A or B antigens.
96.
Procedure:
Asmall drop of the blood sample is placed on a glass slide or in
separate wells of a test plate.
Anti-A serum is added to one drop of blood, and anti-B serum is
added to another.
Observation: The blood is mixed with the reagents, and the
reactions are observed:
If the blood contains antigen A, it will react with the anti-A
antibody, leading to agglutination (clumping of red blood
cells).
If the blood contains antigen B, it will react with the anti-B
antibody, also causing agglutination.
If no agglutination occurs with either reagent, the blood group
is O (since it has neither A nor B antigens).
97.
If theblood has antigen A, it will clump when mixed with
anti-A antibody.
If the blood has antigen B, it will clump when mixed with
anti-B antibody.
If there is no clumping with either antibody, the blood
type is O (because it has neither A nor B antigens).
For AB blood group, the red blood cells have both A
antigens and B antigens.
When mixed with anti-A antibody, the blood will clump
(because of the A antigens).When mixed with anti-B
antibody, the blood will also clump (because of the B
antigens).
So, AB blood group reacts with both anti-A and anti-B
antibodies, showing clumping in both tests.
98.
Example ofBlood Group Determination:
Let's consider someone’s blood sample and how the blood
group is determined:
Step 1: Testing for ABO Blood Group
Blood sample: A person’s blood is tested with anti-A and
anti-B reagents:
Agglutination occurs with anti-A serum, but not with
anti-B serum.
This means the person has A antigens on their red
blood cells, so their blood group is A.
99.
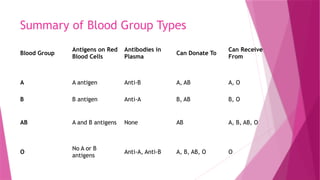
Summary of BloodGroup Types
Blood Group
Antigens on Red
Blood Cells
Antibodies in
Plasma
Can Donate To
Can Receive
From
A A antigen Anti-B A, AB A, O
B B antigen Anti-A B, AB B, O
AB A and B antigens None AB A, B, AB, O
O
No A or B
antigens
Anti-A, Anti-B A, B, AB, O O
100.
Rh BLOOD GROUPSYSTEM
The Rh blood group system is one of the major blood
group systems, and it is based on the presence or absence
of certain proteins on the surface of red blood cells. The
most important of these proteins is the Rh factor, often
referred to as Rh antigen or D antigen. The system is
mainly used to determine whether a person's blood type is
Rh-positive or Rh-negative.
101.
Rh Factor (Dantigen):
The Rh factor is a protein that can either be present or
absent on the surface of red blood cells.
If a person has the Rh factor, they are classified as Rh-
positive (Rh+).
If the Rh factor is absent, they are classified as Rh-
negative (Rh-).
102.
Reticuloendothelial System (RES)
The Reticuloendothelial System (RES), also known as the
Mononuclear Phagocyte System (MPS), refers to a
network of cells and organs in the body that are primarily
responsible for the phagocytosis (engulfing and digesting)
of foreign particles, dead cells, and microorganisms. This
system plays a crucial role in immunity, inflammation, and
the maintenance of tissue homeostasis.
103.
Key Components ofthe Reticuloendothelial System
1. Phagocytic Cells:
Macrophages: These are large, long-lived cells that are
found in various tissues throughout the body. They are
responsible for engulfing and digesting foreign particles,
dead cells, and pathogens. Macrophages are present in
tissues such as the liver (Kupffer cells), lungs (alveolar
macrophages), spleen, lymph nodes, and bone marrow.
Monocytes: These are the precursor cells to macrophages.
Monocytes circulate in the bloodstream and migrate to
tissues where they differentiate into macrophages or
dendritic cells.
104.
Dendritic Cells:These cells are specialized for antigen
presentation and are crucial for activating T-cells in the
immune system.
Kupffer Cells: These are specialized macrophages in the
liver that help in filtering out pathogens and worn-out red
blood cells.
105.
2. Organs Involvedin the RES:
Bone Marrow: The site of production for monocytes and
other blood cells.
Spleen: Filters blood, removing old red blood cells and
pathogens. The spleen houses macrophages that help in
the immune response.
Lymph Nodes: Act as a filtering system, capturing and
processing pathogens and cellular debris, and are sites for
immune activation.
Liver: The liver, through its Kupffer cells, plays an
essential role in filtering and detoxifying blood coming
from the digestive system.
Lungs: Alveolar macrophages in the lungs help protect
against airborne pathogens.
106.
Functions of theReticuloendothelial System
Phagocytosis: The primary function is to engulf and
destroy pathogens, debris, and dead cells.
Immune Response: RES plays a key role in initiating and
regulating immune responses by presenting antigens to
lymphocytes and secreting various cytokines to modulate
the immune system.
Clearance of Waste: Macrophages in the liver, spleen, and
bone marrow clear out old or damaged red blood cells and
other cellular debris.
107.
Functions of theReticuloendothelial System
Iron Recycling: When red blood cells are broken down,
macrophages recycle iron from hemoglobin, which is then
used to produce new red blood cells.
Storage of Cells and Particles: Some cells of the RES,
especially in the spleen, store foreign particles or cells
that are too large to be broken down immediately.
108.
Immunity
Immunity isthe body’s ability to defend itself against
harmful pathogens such as bacteria, viruses, fungi, and
parasites, as well as cancerous cells or foreign substances.
The immune system is a complex network of cells, tissues,
and organs that work together to protect the body from
these threats. It can be broadly classified into two main
types: innate immunity and adaptive immunity.
109.
Types of Immunity
1.Innate Immunity (Non-Specific Immunity)
Definition: This is the body's first line of defense, which is
present at birth and provides immediate, but general
protection against a wide variety of pathogens.
Characteristics:
Non-specific: It does not target specific pathogens;
instead, it reacts to common features shared by many
pathogens.
Immediate response: It acts rapidly upon the first
exposure to a pathogen.
110.
Components:
PhysicalBarriers: Skin, mucous membranes, and cilia in the
respiratory tract help prevent the entry of pathogens.
Chemical Barriers: Enzymes (like lysozyme in saliva), stomach acid,
and antimicrobial peptides kill or inhibit pathogens.
Cells Involved:
Phagocytes: These include neutrophils and macrophages that
ingest and digest pathogens.
Natural Killer (NK) Cells: These cells target and destroy infected
or abnormal cells.
Dendritic Cells: They capture and present antigens to activate
adaptive immunity.
Inflammatory Response: Redness, heat, swelling, and pain at
infection sites due to increased blood flow and immune cell activity.
Complement System: A series of proteins that help enhance immune
responses by promoting inflammation and directly destroying
pathogens.
111.
2. Adaptive Immunity(Specific Immunity)
Definition: Adaptive immunity is the body's second line of
defense and is highly specific to the particular pathogen.
It is slower to respond but provides long-lasting protection
and memory.
Characteristics:
Specificity: It targets specific antigens (foreign
molecules) present on pathogens.
Memory: After the initial exposure, the adaptive
immune system "remembers" the pathogen, making
subsequent responses faster and stronger.
112.
Components:
HumoralImmunity (B Cells): Mediated by B lymphocytes (B cells) that
produce antibodies. Antibodies are proteins that specifically
recognize and bind to antigens, marking them for destruction or
neutralization.
Cell-Mediated Immunity (T Cells): Involves T lymphocytes (T cells),
which directly attack infected cells or regulate the activity of other
immune cells. There are two main types:
Helper T Cells (Th): These help activate B cells and cytotoxic T
cells by releasing signaling molecules (cytokines).
Cytotoxic T Cells (Tc): These directly kill infected or cancerous
cells.
Antigen Presentation: Dendritic cells and macrophages present
antigens to T cells to initiate the adaptive immune response.
113.
Active Immunity vs.Passive Immunity
Active Immunity: The body actively generates its own
immune response, often through exposure to a pathogen
or through vaccination. This process results in the
production of antibodies and memory cells, providing
long-term protection.
Examples:
Natural Immunity: After an individual is infected with
a pathogen, the immune system produces a response
that leads to immunity against future infections from
the same pathogen.
Vaccination: Vaccines introduce a harmless form of a
pathogen (or part of it) to stimulate the immune
system and promote the production of antibodies and
memory cells.
114.
Active Immunity vs.Passive Immunity
Passive Immunity: This occurs when a person receives
pre-formed antibodies from another source, such as from
mother to child via the placenta or breast milk, or through
antibody treatments. Passive immunity provides
temporary protection but does not create memory.
Examples:
Maternal Antibodies: Antibodies passed from mother to
fetus through the placenta, providing protection to the
newborn.
Immunoglobulin Therapy: The injection of antibodies
from donors to provide temporary protection against
infections.
115.
Key Cells inImmunity
1. Lymphocytes:
B Cells: Produce antibodies and are essential for humoral immunity.
T Cells: Help in cell-mediated immunity, with subtypes including
helper T cells (Th) and cytotoxic T cells (Tc).
2. Macrophages: These are large phagocytic cells that engulf and digest
pathogens and debris, and also help activate adaptive immunity by
presenting antigens to T cells.
3. Dendritic Cells: These cells capture antigens and present them to T
cells, initiating the adaptive immune response.
4. Neutrophils: These are the most abundant type of white blood cells
and are the first responders to infection, primarily involved in
phagocytosis.
5. Natural Killer (NK) Cells: These are part of the innate immune
response and target infected or cancerous cells.
116.
Immune Response Stages
Recognition: The immune system recognizes foreign
invaders (such as pathogens or abnormal cells) via
antigens (molecules on the surface of pathogens).
Activation: The immune cells are activated, and signaling
molecules (cytokines) are released.
Effector Response: Effector cells like B cells (producing
antibodies) and cytotoxic T cells (killing infected cells)
perform their tasks.
Memory Formation: After an infection or vaccination,
memory cells are formed, ensuring faster and stronger
responses in future exposures.
117.
Immunological Disorders
AutoimmuneDiseases: The immune system mistakenly
attacks healthy cells and tissues, such as in rheumatoid
arthritis and multiple sclerosis.
Immunodeficiency: When the immune system is
weakened, either due to genetic disorders (e.g., SCID –
Severe Combined Immunodeficiency) or acquired
conditions like HIV/AIDS, the body becomes more
susceptible to infections.
Allergies: Overreaction of the immune system to harmless
substances (allergens) such as pollen or pet dander,
leading to conditions like asthma or hay fever.
118.
1. MCV(Mean Corpuscular Volume)
Definition: MCV is a measure of the average volume (size)
of individual red blood cells.
Unit: It is usually measured in femtoliters (fL).
Normal Range: 80-100 fL (this can vary slightly depending
on the lab or age).
Low MCV (<80 fL)
Normal MCV (80-100 fL)
High MCV (>100 fL)
119.
2. MCH(Mean Corpuscular Hemoglobin)
Definition: MCH is a measure of the average amount of
hemoglobin present in a single red blood cell.
Unit: It is measured in picograms (pg).
Normal Range: 27-33 pg (again, this can vary slightly by
lab or age).
Low MCH (<27 pg)
Normal MCH (27-33 pg)
High MCH (>33 pg)
MCV focuses on the size of red blood cells, while MCH
focuses on the hemoglobin content within each cell.
120.
DISORDERS OF BLOOD
Disorders of blood refer to a variety of conditions
that affect the components of the blood,
including red blood cells, white blood cells,
platelets, plasma, and clotting factors. These
disorders can affect blood circulation, oxygen
delivery, immune system function, and clotting
ability.
121.
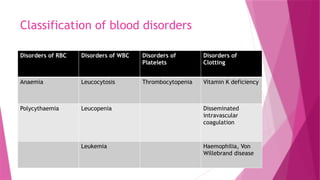
Classification of blooddisorders
Disorders of RBC Disorders of WBC Disorders of
Platelets
Disorders of
Clotting
Anaemia Leucocytosis Thrombocytopenia Vitamin K deficiency
Polycythaemia Leucopenia Disseminated
intravascular
coagulation
Leukemia Haemophilia, Von
Willebrand disease
122.
Disorders of erythrocytes
1.ANAEMIA:is defined as decreased oxygen
carrying capacity of blood. Anemia occurs
when there is a shortage of red blood cells
or hemoglobin in the blood, leading to
reduced oxygen delivery to tissues and
organs.
123.
TYPES OF ANAEMIA
MORPHOLOGICALCLASSIFICATION:
Anemia on the basis of size of RBCs: it is judged by mean
corpuscular volume (MCV) and is classified as
1. Normocytic Anemia: In this type of anemia, the red
blood cells are of normal size (mean corpuscular volume or
MCV between 80-100 fL). However, the number of red blood
cells is reduced.
2. Microcytic Anemia:The red blood cells are smaller than
normal (MCV < 80 fL). The RBCs may also appear pale
(hypochromic).
3. Macrocytic Anemia: The red blood cells are larger than
normal (MCV > 100 fL), often due to defective DNA synthesis
in the bone marrow.
124.
TYPES OF ANAEMIA
MORPHOLOGICALCLASSIFICATION:
Anemia on the basis of amount of hemoglobin per RBC:
it is determined by mean corpuscular hemoglobin (MCH)
and is classified as
1. Hypochromic anemia: red blood cells have a lower
hemoglobin content i.e., MCH less than normal
2. Normochromic anemia: red blood cells have a normal
amount of hemoglobin. i.e., MCH is normal
3. Hyperchromic anemia: red blood cells have more
hemoglobin than normal i.e., MCH is more than normal
125.
TYPES OF ANAEMIA
ETIOLOGICALCLASSIFICATION(Based on the cause):
Anemia caused by blood loss:
_ Posthaemorrhagic anemia
_Haemolytic anaemia
Anaemia due to defective blood formation:
_Nutritional Anemia (iron deficiency, protein deficiency,
lack of folic acid, vitamin C, B12 deficiency)
_Lack or failure of absorption: B12 deficiency anaemia
caused due to lack of intrinsic factor of the stomach
_Aplasia of bone marrow: failure of bone marrow to
function due to poisoning radiation (by X rays, gamma rays),
renal diseases, etc.
126.
1. Posthaemorrhagic Anemia:
This type of anemia occurs after significant blood loss
(hemorrhage), whether acute (rapid) or chronic (slow,
ongoing). When a large amount of blood is lost, the body’s
ability to produce enough red blood cells to replace the
lost volume is impaired, leading to a decrease in red blood
cell count and hemoglobin levels.
Causes: Trauma, surgery, gastrointestinal bleeding, heavy
menstruation, or conditions causing internal bleeding.
Symptoms: Fatigue, weakness, dizziness, and pallor.
Treatment: Treatment typically involves blood
transfusions, iron supplements, and addressing the
underlying cause of bleeding.
127.
2. Hemolytic Anemia:
This type of anemia occurs when red blood cells are destroyed
(hemolysis) faster than they can be produced by the bone
marrow. This leads to a reduced number of red blood cells in
circulation.
Causes: Hemolytic anemia can be caused by inherited
conditions (e.g., sickle cell disease, thalassemia), autoimmune
disorders (where the body attacks its own red blood cells),
infections, or exposure to certain toxins or medications.
Symptoms: Symptoms include jaundice (yellowing of the skin
and eyes), fatigue, dark-colored urine, and an enlarged spleen
or liver.
Treatment: Treatment depends on the underlying cause and
may include steroids, immune-suppressing drugs, or blood
transfusions. In some cases, removal of the spleen
(splenectomy) may be recommended.
128.
IRON DEFICIENCY ANEMIA
It is the most common anemia in many parts of the world.
It is microcytic, hypochromic type of anemia.
It is mainly due to nutritional deficiency of iron
Common symptoms include:
Fatigue and general weakness
Paleness of the skin or the inside of the lower eyelids
Shortness of breath and dizziness, especially during physical activity
Cold hands and feet
Headaches
Brittle nails or hairloss
Cravings for non-nutritive substances (like ice, dirt, or starch), a
condition called pica
129.
Causes of IronDeficiency Anaemia
Inadequate Iron Intake: A diet lacking in iron-rich foods
(such as red meat, leafy green vegetables, beans, and
fortified cereals) can lead to iron deficiency, especially if
the body’s iron demands increase.
Increased Iron Requirements:-Certain life stages increase
the body's need for iron, such as:
1. Pregnancy (due to increased blood volume and the need
to supply iron to the developing fetus)
2. Infancy and childhood (when growth and development
require more iron)
3. Menstruating women (who lose iron through menstrual
blood)
130.
Causes of IronDeficiency Anaemia
Blood Loss: Chronic blood loss, such as from
gastrointestinal bleeding (e.g., ulcers, hemorrhoids, or
colorectal cancer), heavy menstrual periods, or frequent
blood donations, can lead to iron deficiency.
Poor Iron Absorption: Certain medical conditions or
medications may interfere with the absorption of iron,
such as: Celiac disease, Crohn’s disease, Gastric bypass
surgery, Use of antacids or proton pump inhibitors (which
reduce stomach acid)
131.
Treatment of IronDeficiency Anaemia
Iron Supplements: The most common treatment for iron
deficiency anaemia is oral iron supplements (ferrous
sulfate or ferrous gluconate).
Dietary Changes: Increasing iron-rich foods in the diet is
important. Foods high in iron include: Red meat, poultry,
fish, and shellfish, Leafy green vegetables (e.g., spinach,
kale),Beans, lentils, tofu, Fortified cereals and grains,
Nuts and seeds
Intravenous Iron Therapy: In severe cases or when oral
iron supplements are not effective or cause side effects,
intravenous (IV) iron may be administered in a hospital or
clinic.
132.
Treatment of IronDeficiency Anaemia
Treating Underlying Conditions: If the iron deficiency is
due to an underlying medical condition (e.g., bleeding
ulcer, celiac disease), addressing that condition is key to
resolving the anaemia.
Blood Transfusions (In Severe Cases): For very severe
anaemia or in cases where iron therapy is not effective, a
blood transfusion may be necessary to quickly restore
healthy red blood cells.
133.
Megaloblastic anaemia
Megaloblasticanaemia is a type of anaemia
characterized by the presence of abnormally large
red blood cells (megaloblasts) in the bone marrow
and blood. These oversized cells are immature
and dysfunctional, leading to ineffective red
blood cell production. It is typically caused by a
deficiency in either vitamin B12 or folate, both
of which are essential for the production and
maturation of red blood cells.
134.
Pernicious Anaemia
Perniciousanemia is a type of anemia caused by
a deficiency of vitamin B12, which is necessary for
the production of red blood cells. It occurs when
the body cannot absorb enough vitamin B12 from
the digestive tract. This condition is often due to
an autoimmune disorder where the body's immune
system attacks the cells in the stomach that
produce intrinsic factor, a protein needed for
vitamin B12 absorption.
Megaloblastic anemia caused by deficiency of
vitamin B12 is termed as pernicious anemia.
135.
Without enough vitaminB12, the body cannot produce
enough healthy red blood cells, leading to the symptoms of
anemia. These can include:
Fatigue
Weakness
Pale skin
Shortness of breath
Dizziness
Numbness or tingling in the hands and feet (due to nerve
damage)
Cognitive difficulties, such as memory problems or
confusion
136.
Causes of perniciousanemia
Autoimmune response: The most common cause of
pernicious anemia is an autoimmune reaction that affects
the stomach lining and intrinsic factor production.
Dietary deficiency: In rare cases, pernicious anemia can
be caused by a lack of B12 in the diet, particularly in
people who follow vegetarian or vegan diets, as vitamin
B12 is primarily found in animal products.
Other conditions: Certain gastrointestinal conditions, such
as Crohn's disease, gastric surgery, or infections, can also
lead to a decreased ability to absorb vitamin B12.
137.
Treatment
Treatment for perniciousanemia usually involves:
Vitamin B12 injections: The most common treatment to
bypass the need for intrinsic factor in absorption.
Oral B12 supplements: High-dose oral B12 may be
effective if the body can absorb it, particularly in milder
cases.
Dietary changes: If the condition is related to dietary
deficiency, increasing B12-rich foods or taking
supplements can help.
138.
APLASTIC ANAEMIA
Aplasticanemia is a rare but serious condition where the
bone marrow fails to produce enough new blood cells. This
leads to a deficiency in red blood cells, white blood cells,
and platelets, which can result in a variety of symptoms
related to these deficiencies, such as:
Symptoms:
Fatigue: Due to a low red blood cell count, leading to
decreased oxygen delivery to tissues.
Paleness: A result of the reduced number of red blood
cells.
Frequent infections: Due to a low white blood cell count
(leukopenia), making it harder for the body to fight off
infections.
139.
APLASTIC ANAEMIA
Symptoms:
Easy bruising or bleeding: A low platelet count
(thrombocytopenia) can cause spontaneous bruising,
nosebleeds, and gum bleeding.
Shortness of breath: Again, due to a lack of red blood
cells and oxygen transport.
Dizziness or lightheadedness: Caused by low blood cell
counts.
140.
Causes of Aplasticanemia
Autoimmune reactions: The most common cause, where the
body's immune system mistakenly attacks the bone marrow.
Infections: Certain viral infections, such as hepatitis, Epstein-
Barr virus, and HIV, can damage the bone marrow.
Chemicals and drugs: Certain medications (like chemotherapy
drugs or antibiotics), as well as exposure to toxic chemicals
such as benzene, can lead to aplastic anemia.
Radiation: Exposure to high levels of radiation can damage bone
marrow.
Pregnancy: A rare form of acquired aplastic anemia can occur
during pregnancy, particularly in the second trimester.
Fanconi anemia: A genetic disorder that leads to bone marrow
failure.
Other inherited conditions: Some rare genetic conditions can
lead to aplastic anemia.
141.
Haemolytic anaemias
Hemolyticanemia is a type of anemia that occurs
when red blood cells are destroyed (hemolysis)
faster than the bone marrow can produce them.
The rapid breakdown of red blood cells leads to a
shortage of these cells in the bloodstream,
causing the symptoms of anemia. Hemolytic
anemia can be either acquired or hereditary and
can occur in various forms.
142.
Types of HemolyticAnemia
1. Acquired Hemolytic Anemia:
Autoimmune Hemolytic Anemia (AIHA): In this condition, the body’s
immune system mistakenly attacks and destroys its own red blood
cells.
Infections: Certain infections, particularly malaria, can cause
hemolysis.
Medications: Some drugs, such as penicillin or certain chemotherapy
agents, can cause hemolytic anemia.
Toxins and chemicals: Exposure to toxic substances or chemicals
(e.g., snake venom or some industrial chemicals) can lead to
hemolysis.
Mechanical causes: Prosthetic heart valves, hemodialysis, or other
mechanical devices can physically damage red blood cells.
Hypersplenism: An overactive spleen can destroy red blood cells
faster than normal.
143.
Types of HemolyticAnemia
2. Hereditary Hemolytic Anemia:
Sickle Cell Anemia: A genetic disorder where the red
blood cells are abnormally shaped (sickle-shaped), making
them fragile and prone to breaking apart.
Thalassemia: A group of inherited blood disorders where
the body produces abnormal hemoglobin, leading to the
premature destruction of red blood cells.
144.
Symptoms
The symptoms ofhemolytic anemia result from the rapid
destruction of red blood cells and the body's inability to replace
them quickly enough. These include:
Fatigue or weakness
Paleness or jaundice (yellowing of the skin and eyes)
Dark-colored urine (from the release of hemoglobin into the
bloodstream)
Shortness of breath
Rapid heart rate (tachycardia)
Enlarged spleen (splenomegaly) and/or liver (hepatomegaly) in
some cases, due to increased processing of destroyed cells
Abdominal pain (in cases of splenomegaly)
145.
Treatment
Treatment for hemolyticanemia depends on the underlying cause:
Acquired Hemolytic Anemia:
Corticosteroids: In cases of autoimmune hemolytic anemia,
steroids like prednisone are often used to suppress the
immune system.
Immunosuppressive drugs: Drugs like azathioprine or
rituximab may be used if steroids are not effective.
Blood transfusions: In severe cases of hemolysis, blood
transfusions may be needed to replace lost red blood cells.
Splenectomy: In cases of hereditary spherocytosis or if the
spleen is overactive, surgical removal of the spleen may be
necessary.
146.
Treatment
Hereditary HemolyticAnemia:
Sickle Cell Anemia: Treatment may include pain
management, blood transfusions, hydroxyurea (a
medication that increases fetal hemoglobin production),
and in severe cases, bone marrow/stem cell transplants.
Thalassemia: Regular blood transfusions and iron
chelation therapy (to prevent iron overload) are often
needed.
147.
Prognosis
The prognosis forhemolytic anemia varies depending on its cause:
Acquired forms: If treated promptly, many acquired forms of
hemolytic anemia can be managed successfully. However, if left
untreated or in severe cases, it can lead to complications such
as organ failure.
Hereditary forms: The prognosis for hereditary hemolytic
anemia can vary. Some individuals with milder forms (e.g.,
hereditary spherocytosis) may live relatively normal lives with
few symptoms, while others (e.g., sickle cell disease) may
experience severe complications, but treatment can help
manage symptoms and improve quality of life.
148.
Polycythemia
Polycythemia isa condition characterized by an
increased number of red blood cells in the
bloodstream, leading to thicker blood. This
increased blood viscosity can impair circulation
and oxygen delivery to tissues. Polycythemia can
be classified into two main types: primary and
secondary.
149.
Primary Polycythemia (PolycythemiaVera)
Polycythemia vera (PV) is a rare, chronic blood disorder
in which the bone marrow produces an excessive amount
of red blood cells.
In this RBC count is more than 7-8 million/mm³.
There is also excess production of WBCs and platelets.
An increase in RBC count to a high level causes an
increase in the viscosity of blood and an increase in
peripheral resistance, leading to an increase in blood
pressure.
The increase in viscosity also reduces the rate of blood
flow in vessels.
It can lead to coronary and cerebral thrombosis.
150.
Secondary Polycythemia
Secondarypolycythemia occurs when there is an
increase in erythropoietin (EPO), the hormone
responsible for stimulating the production of red
blood cells. This is usually in response to low oxygen
levels in the blood (hypoxia).
Hypoxia stimulates erythropoietin secretion, which
stimulates erythropoiesis.
Thus, exposure to chronic hypoxia causes
polycythemia.
Such polycythemia can be seen in a native of high
altitude.
151.
DISORDERS OF LEUCOCYTES
1. Leukocytosis:
Leukocytosis is a condition where there is an
increased number of white blood cells (WBCs) in
the blood, typically above 11,000 cells per
microliter. It often indicates an infection,
inflammation, or a response to stress, injury, or
other underlying conditions.
152.
Causes:
Infections(bacterial, viral, fungal)
Inflammatory diseases (e.g., rheumatoid
arthritis)
Leukemia (a form of blood cancer)
Stress (physical or emotional)
Medications (e.g., corticosteroids)
Allergic reactions
153.
Symptoms:
Often relatedto the underlying cause (e.g., fever,
fatigue, swelling).
May not cause noticeable symptoms on its own.
Diagnosis:
Blood tests to measure the number of white
blood cells.
Further tests may be conducted to identify the
underlying cause, such as a blood culture,
imaging, or specific tests based on symptoms.
154.
2. Leukopenia:
Leukopenia is the decrease in the number of white blood
cells below the normal range (usually less than 4,000 cells
per microliter). This condition makes the body more
vulnerable to infections.
Causes:
Bone marrow disorders (e.g., aplastic anemia)
Viral infections (e.g., HIV, hepatitis)
Autoimmune diseases (e.g., lupus)
Medications (e.g., chemotherapy, immunosuppressants)
Nutritional deficiencies (e.g., vitamin B12 or folate)
Radiation exposure
155.
Symptoms:
Increasedsusceptibility to infections.
Symptoms related to infections such as fever, chills,
and fatigue.
Diagnosis:
Blood tests to confirm low white blood cell counts.
Additional tests may identify the underlying cause
(e.g., bone marrow biopsy, viral testing).
156.
LEUKEMIA
It isa malignant disease in which the WBC count is greatly
increased and premature WBCs also appear in the
peripheral circulation.
In leukemia, the bone marrow produces too many WBCs,
but these are usually immature (not fully developed) and
non-functional.
These abnormal cells are often called "blasts.“
In leukemia, immature or premature WBCs (blasts) spill
over into the peripheral blood — the blood that circulates
through the body outside the bone marrow. These blasts
can't function properly and crowd out healthy blood cells.
This disrupts normal blood function and weakens the
immune system.
157.
The exactcauses of leukemia are mostly
unknown.
Main Causes / Risk Factors of Leukemia:
1. Genetic Mutations
Changes (mutations) in the DNA of blood cells can
cause them to grow uncontrollably.
These mutations may occur spontaneously or be
inherited.
2. Radiation Exposure
High levels of ionizing radiation (like from nuclear
accidents or radiation therapy) can damage bone
marrow and increase leukemia risk.
158.
3. Chemical Exposure
Long-term exposure to certain chemicals like
benzene (used in industry) is linked to some types
of leukemia.
4. Previous Cancer Treatments
People who have had chemotherapy or radiation
for other cancers have a higher risk of developing
secondary leukemia.
In leukemia, there is an uncontrolled
production of WBCs by cancerous multiplication
of a myelogenous cell or lymphogenous cell.
159.
1. Myelogenous(Myeloid) Cells
These are immature cells in the bone marrow that
develop into:
Neutrophils
Basophils
Eosinophils
Monocytes
And also red blood cells and platelets
When leukemia starts in these cells, it’s called:
Acute Myeloid Leukemia (AML)
Chronic Myeloid Leukemia (CML)
These types usually affect the production of granulocytes
(a type of WBC), and disrupt normal blood cell production
more broadly.
160.
2. Lymphogenous(Lymphocytic / Lymphoid)
Cells
These are immature cells that become:
Lymphocytes (T cells, B cells, and NK cells)
These cells are part of the immune system.
When leukemia starts in these cells, it’s called:
Acute Lymphoblastic Leukemia (ALL)
Chronic Lymphocytic Leukemia (CLL)
These leukemias mainly affect the immune
defense system and often involve lymph nodes
too.
161.
Type of LeukemiaAffects Which Cells? Acute or Chronic?
AML (Acute Myeloid
Leukemia)
Myeloid cells Acute (fast-growing)
CML (Chronic Myeloid
Leukemia)
Myeloid cells Chronic (slow-growing)
ALL (Acute Lymphoblastic
Leukemia)
Lymphoid cells Acute
CLL (Chronic Lymphocytic
Leukemia)
Lymphoid cells Chronic
162.
HAEMORRHAGIC DISORDERS
Haemorrhagicdisorders are conditions causing
excessive bleeding.
There are three types of disorders that cause
bleeding disorders:
1. Thrombocytopenia
2. Deficiency of vitamin K
3. Haemophilia
163.
Thrombocytopenia
Platelet countless than 50,000/ mm³ is termed as
thrombocytopenia.
Causes of Thrombocytopenia:
Decreased platelet production (in bone marrow)
Leukemia, aplastic anemia, infections, chemotherapy,
radiation
Increased destruction of platelets
Immune system attacks them (e.g., ITP – immune
thrombocytopenic purpura)
Autoimmune diseases (like lupus)
Platelets trapped in the spleen
Enlarged spleen (splenomegaly) holds more platelets
than normal
164.
Symptoms
Easy bruising
Prolonged bleeding from cuts
Petechiae (tiny red/purple spots on the skin)
Bleeding gums or nose
Heavy menstrual periods
Blood in urine or stool (in severe cases)
165.
Treatment
Treatment Dependson the Cause:
Mild cases may need no treatment
Severe cases might need:
Medications (like steroids or immune
suppressants)
Platelet transfusions
Treating the underlying cause (e.g., stopping
a drug or treating an infection)
Spleen removal (splenectomy) in chronic cases
166.
Thrombocytopenic Purpura
Thrombocytopenic= Low platelet count
Purpura = Purple spots on the skin due to bleeding
underneath
When circulating thrombocytes are less in number, there is
a tendency to bleed, especially from small venules and
capillaries. As a result, small punctate haemorrhages
occur in all body tissues. On skin, small, purplish blotches
are seen. This condition is called as thrombocytopenic
purpura.
If bleeding time and clotting time are measured, it is seen
that bleeding time is prolonged but clotting time remains
normal.
167.
Deficiency of VitaminK
Vitamin K is essential for the production of clotting
factors II, VII, IX and X in the liver. Therefore deficiency
of vitamin K leads to bleeding disorder.
It can occur in newborns or adults.
In newborns, the deficiency is common because vitamin K
does not cross the placenta efficiently, their intestines
lack the bacteria needed to produce it, and breast milk
contains only small amounts of the vitamin. Additionally, a
newborn's liver is not fully developed to process vitamin K
properly.
168.
In adults,vitamin K deficiency is much less common
and usually results from fat malabsorption conditions
like celiac disease, Crohn’s disease, or liver disorders,
since vitamin K is a fat-soluble vitamin. It can also
occur due to long-term antibiotic use, which
destroys gut bacteria that help produce vitamin K, or
from a very poor diet. Symptoms in adults include
easy bruising, bleeding gums, nosebleeds, and
blood in urine or stool due to impaired blood
clotting.
Treatment for both adults and newborns involves
vitamin K supplementation, either orally or by
injection, depending on the severity of the
deficiency.
169.
Disseminated Intravascular Coagulation(DIC)
In DIC, the clotting system is triggered throughout the body.
Tiny clots form in the blood vessels, using up the clotting
factors and platelets.
In DIC, the clotting system is overactivated, leading to tiny
clots all over the body. This consumes clotting factors and
platelets, causing a dual problem:
Clots in small blood vessels can damage organs.
Bleeding happens in other places because there are not
enough clotting factors to stop it.
DIC is a complication, not a primary disease.
In DIC, small but numerous clots are formed. They plug a large
share of peripheral blood vessels.
170.
Disseminated Intravascular Coagulation(DIC)
DIC is not a disease itself, but a complication of another
condition, such as:
Severe infections (like sepsis)
Trauma or surgery, especially with significant blood loss
Cancer, particularly leukemia or solid tumors
Pregnancy complications, such as placental abruption or
eclampsia
Severe burns
Severe liver disease
Snake bites (venom causing clotting abnormalities)
171.
Treatment
Addressing theunderlying cause (e.g., treating
infection, surgery, or managing pregnancy
complications).
Supportive care:
Blood transfusions to replenish clotting factors
and platelets
Anticoagulants (like heparin) may be used in
certain cases to stop excessive clotting
IV fluids to maintain blood pressure and organ
function
Fibrinolytic therapy (for cases with excessive clot
formation)
172.
Haemophilia
It isa bleeding disorder in which clotting time is
prolonged but bleeding time remains normal.
It results due to deficiency of clotting factor, either
factor VIII or factor IX.
It is of two types:
1. Haemophilia A : it is due to deficiency of factor VIII
(anti haemophillic factor).
2. Haemophilia B ( Christmas disease): it is less common
and is due to deficiency of factor IX.
173.
1. Hemophilia A:
Cause: Hemophilia A is caused by a deficiency or dysfunction
of Factor VIII (also known as anti-hemophilic factor).
Inheritance: It is an X-linked recessive condition, which means
it primarily affects males and is passed through females
(carriers).
Effect: Factor VIII is a critical component of the clotting
cascade, and without it, the blood cannot form a proper clot.
This leads to excessive bleeding, especially after injury or
surgery.
Symptoms of Hemophilia A:
Easy bruising
Spontaneous bleeding in joints and muscles
Prolonged bleeding from cuts or injuries
174.
2. Hemophilia B(Christmas Disease):
Cause: Hemophilia B is due to a deficiency of Factor IX
(also known as Christmas factor).
Inheritance: Like Hemophilia A, Hemophilia B is also X-
linked recessive and primarily affects males.
Effect: Factor IX plays a crucial role in the coagulation
cascade, and without it, the blood can't clot properly,
leading to similar bleeding issues as in Hemophilia A.
Symptoms of Hemophilia B:
Similar to Hemophilia A: easy bruising, joint bleeding,
and prolonged bleeding.
Editor's Notes
#2 a measure of the density of a substance in comparison to the density of water. It is a dimensionless quantity, meaning it has no units, and is simply a ratio.
If SG > 1: The substance is denser than water and will sink if placed in water.
If SG < 1: The substance is less dense than water and will float.
If SG = 1: The substance has the same density as water and will neither sink nor float.
(SG) of blood typically ranges between 1.050 and 1.060. This means that blood is slightly denser than water, which has a specific gravity of 1.
#3 straw color comes primarily from bilirubin, a breakdown product of hemoglobin from red blood cells. The concentration of bilirubin is usually low, which gives plasma its yellowish tint. It is considered normal and healthy for plasma to have this color.
plasma refers to the pale yellow appearance of the liquid portion of blood when it is separated from the red blood cells, white blood cells, and platelets.
Blood plasma contains essential trace elements like zinc, chromium, copper, selenium, manganese, nickel, arsenic, cobalt, molybdenum, iodine, and magnesium
Clotting factors are proteins in the blood that work together to form a blood clot. This process is known as coagulation and helps stop bleeding when blood vessels are injured. There are 13 major clotting factors (labeled I to XIII)
#5 PCV is the percentage of blood that is made up of red blood cells.
#19 density of blood refers to the mass of blood per unit volume
#33 Blood cell lineages refer to the developmental pathways of blood cells, originating from a single type of stem cell (hematopoietic stem cell) and differentiating into various specialized blood cell types like red blood cells, white blood cells, and platelets.
#40 Quaternary protein structure refers to the highest level of protein organization, where multiple polypeptide chains (subunits) come together to form a functional protein complex.
#42 In sickle cell disease, a mutation in the beta chains of hemoglobin causes the hemoglobin to stick together in low oxygen conditions. This makes red blood cells change shape into a sickle, which can block blood flow and cause pain.
#47 EPO boosts RBC production when oxygen levels in the blood are low.
#51 Polycythemia is a blood disorder that occurs when there are too many red blood cells in the body. This makes the blood thicker and less able to flow through blood vessels and organs.
#54 Histamine is a chemical involved in several important bodily functions, especially in the immune system and during allergic reactions.
Diphenhydramine (Benadryl)
Loratadine (Claritin), Cetirizine (Zyrtec) , Fexofenadine (Allegra)
Chlorpheniramine (Chlor-Trimeton)
These medications work by blocking histamine receptors, reducing symptoms like sneezing, itching, and swelling that occur during allergic reactions.
#65 1.5 lac to 4.5 lac per millimeter cube of blood.
#72 cascade" refers to a series of events or reactions where one event triggers the next
#75 Factor VII SERUM PROTHROMBIN CONVERSION ACCELERATOR
The "a" denotes that Factor IX has undergone activation, meaning it has been converted from an inactive form into its active, enzymatically functional form.
#76 PLASMA THROMBOPLASTIN COMPONENT (Christmas Factor)
Stephen Christmas was born in the 1950s and diagnosed with a bleeding disorder known as hemophilia B, also called Christmas disease. This condition was characterized by a deficiency in Factor IX, which impairs the blood's ability to clot properly.
In 1952, researchers identified the deficiency of Factor IX in Christmas' blood, and thus, the clotting factor was named Christmas Factor in his honor.
#77 The "a" denotes that Factor IX has undergone activation, meaning it has been converted from an inactive form into its active, enzymatically functional form.
#78 The "a" denotes that Factor IX has undergone activation, meaning it has been converted from an inactive form into its active, enzymatically functional form.
#81 Serotonin is a neurotransmitter but also functions as a vasoconstrictor in platelets.
chemical messengers that transmit signals between neurons (nerve cells) and other cells
Serotonin: Plays a role in mood, sleep, and appetite.
#88 Clotting time is the time it takes for blood to stop flowing and form a clot after a vessel is injured. It's the period between when blood starts to ooze out and when it forms a solid clot to stop the bleeding.
#125 occurs when the body cannot produce enough healthy red blood cells (RBCs), often due to problems in the bone marrow or issues with the production of hemoglobin.
#130 Celiac Disease is primarily a reaction to gluten that affects the small intestine, while Crohn’s Disease is a broader inflammatory condition of the GI tract that can affect any part of it. Celiac disease primarily causes iron deficiency by damaging the small intestine and impairing iron absorption.
Crohn’s disease can cause iron deficiency due to both impaired absorption and intestinal bleeding, often complicated by chronic inflammation.
Celiac disease can be controlled by a gluten-free diet, while Crohn’s disease requires a combination of medication and sometimes surgery for management.
#149 Thrombosis refers to the formation of a blood clot (thrombus) within a blood vessel, which can obstruct the flow of blood
#150 More red blood cells (RBCs) are produced and released into the bloodstream.
These RBCs carry more oxygen, gradually correcting the hypoxia.
Hypoxia → HIF-1α activation in kidneys → ↑ EPO production → Bone marrow stimulation → ↑ RBCs → ↑ Oxygen delivery → EPO production decreases
hypoxia-inducible factors (HIFs)
#156 malignant tumor is cancer. It tends to Grow aggressively, Invade nearby tissues,Spread to other parts of the body (metastasize) e.g. Lung cancer, breast cancer, leukemia
Opposite of malignant = benign
A benign tumor doesn’t spread and is usually less dangerous. Lipoma (fat tumor), uterine fibroids, skin moles
#158 Benzene – found in gasoline, solvents, and some industrial environments
#161 acute refers to conditions that have a sudden onset, are of short duration, and can be treated or cured. Chronic refers to conditions that develop slowly, last for a long period (often years or even a lifetime), and may not be fully curable, but can often be managed.
#166 Capillaries and venules are fragile, and they naturally get micro-damage (especially from movement, pressure, inflammation, etc.)
If there aren't enough platelets, small vessels leak, leading to internal bleeding and visible skin spots (purpura).
#167 Factor II Prothrombin
Factor VII (Proconvertin or Stable Factor
Factor IX (Christmas Factor
Factor X (Stuart-Prower Factor
#168 Vitamin K is a fat-soluble vitamin, meaning it dissolves in fat and is stored in the body’s fat tissues and liver.
Celiac disease (damages the small intestine)
Crohn's disease (inflammatory bowel disease)
Liver disorders (liver makes some of the proteins needed for clotting)
#169 peripheral blood vessels (the small vessels far from the heart, such as capillaries and venules).
#170 Placental abruption happens when the placenta (the organ that nourishes the baby in the womb) separates prematurely from the uterine wall.
Eclampsia is a condition characterized by high blood pressure and protein in the urine during pregnancy. Eclampsia is the onset of seizures in a pregnant woman with preeclampsia. Both trigger DIC by causing severe bleeding or blood vessel damage.
In both conditions, clotting factors and platelets are consumed too quickly, leading to small clots forming throughout the body and causing organ damage or bleeding.