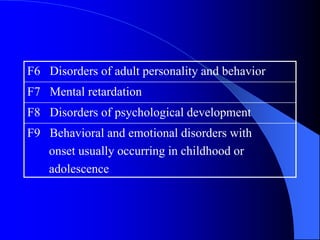
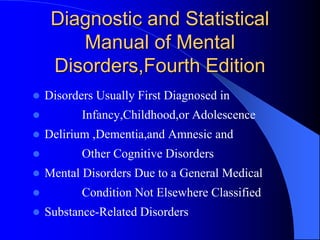
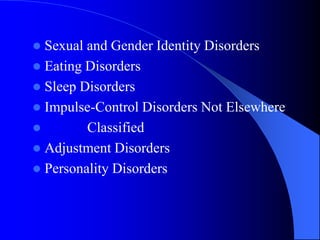
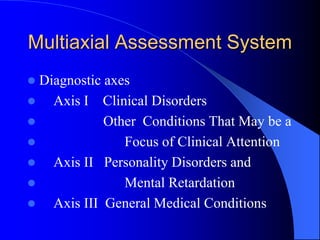
This document discusses the field of psychiatry. It begins by defining psychiatry as the study of the causes, mechanisms, symptoms, prognosis, diagnosis and treatment of mental illnesses. It then discusses the broad scope of conditions studied in psychiatry, from severe psychoses to neuroses and personality disorders. The document also outlines various branches and classifications of psychiatry, diagnostic criteria for mental disorders, and the biological, psychological and social factors that can contribute to psychiatric illnesses.