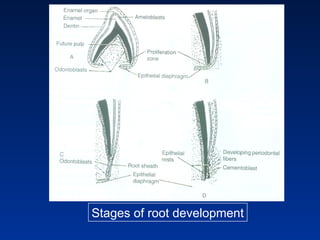
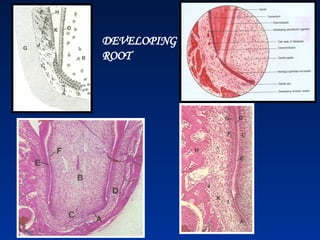
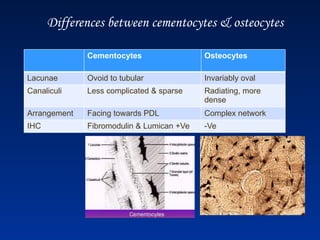
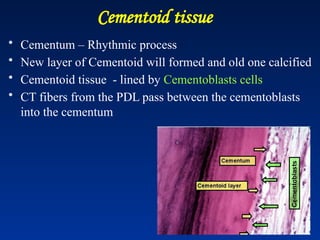
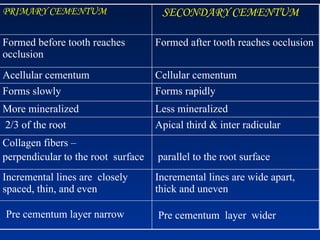
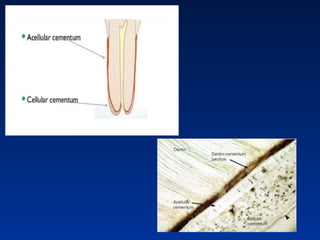
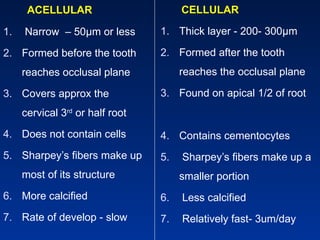
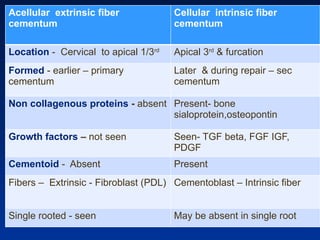
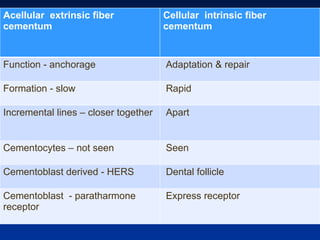
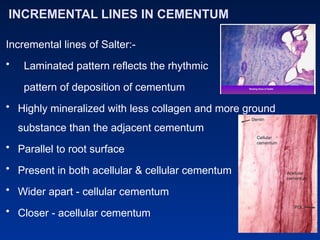
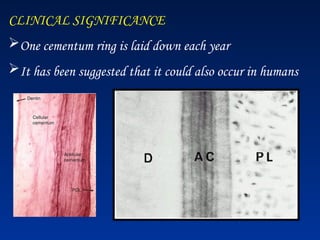
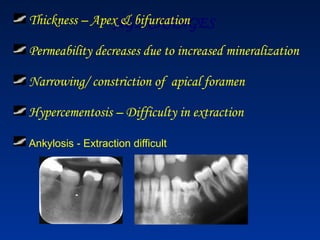
El documento detalla las etapas del desarrollo de las raíces dentales, centrándose en la formación del cemento y la dentina, así como la clasificación del cemento en primario y secundario. Se discuten las características físicas y químicas del cemento, incluyendo su composición orgánica e inorgánica, y su importancia en la función de anclaje y reparación dental. Además, se abordan aspectos clínicos como la hipercementosis y el movimiento ortodóntico de los dientes, junto con los cambios relacionados con la edad en el cemento.


































![general_and_extraoral_examination[1]__-__Read-Only n.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/generalandextraoralexamination1-read-onlyn-250216162540-10c854ca-thumbnail.jpg?width=640&height=640&fit=bounds)





![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)















