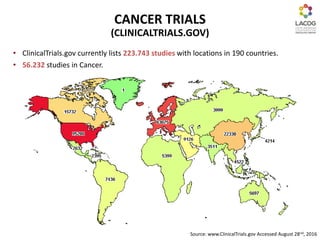
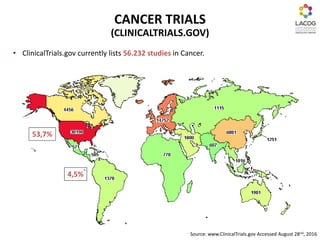
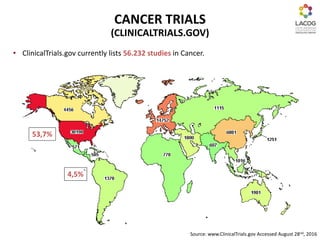
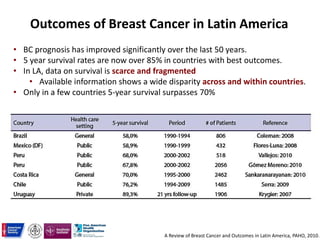
Clinical research is essential to improving cancer treatment results. It offers patients access to state-of-the-art therapies through clinical trials when standard treatments may not be available or adequate. Latin America represents an important region for clinical research due to its large patient populations and qualified investigators. However, barriers like bureaucratic hurdles can stall development. Addressing discrepancies in cancer care globally through strategies like screening programs and vaccination could help reduce the growing cancer burden in developing areas.
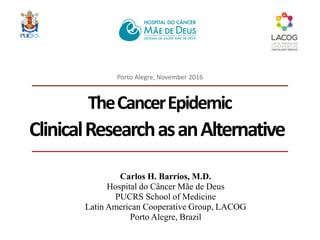
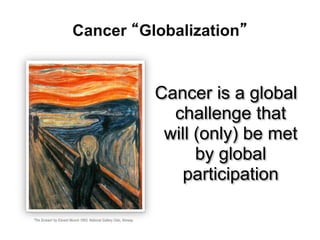
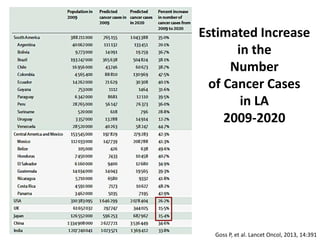
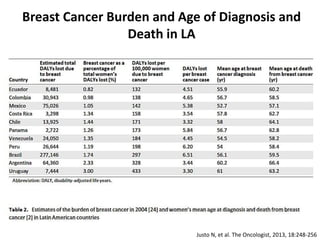
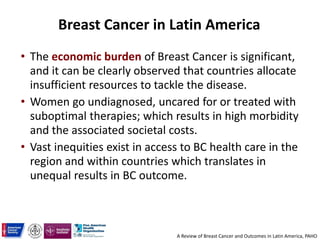
![Breast Cancer: Number of Cases/year 57.120
Cases in the public system-SUS (73.7%) 42.097
Stages I/II/III (94%) 39.571
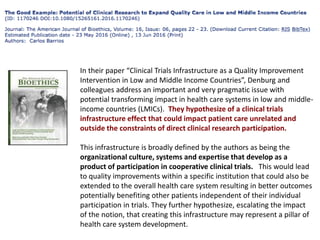
HER2 positive patients (20%) 7.914
Number of deaths avoided by Trastuzumab/y (8.8%) 696
Deaths in HER2 positive women (2005-2012)* 4872
Estimated number of deaths in early HER2 positive patients due
to lack of access to adjuvant Trastuzumab in the public system in
Brazil 2005-2012.
INCA. Câncer de mama. http://www2.inca.gov.br/wps/wcm/connect/tiposdecancer/site/home/mama, Jan 2014.
IBGE. Pesquisa Nacional por Amostra de Domicílios, 2008 [acesso March 2,
2014].http://www.ibge.gov.br/home/estatistica/populacao/panorama_saude_brasil_2003_2008/PNAD_2008_saude.pdfN)
Simon, SD, et al. Projeto Amazona I, GBECAM
Perez E, ate al. J Clin Oncol 32:374, 2014.
* Presumes constant incidence and mortality 2005-2012
Barrios C, et al. JCO, Brazilian Edition, 2015.](https://image.slidesharecdn.com/carloshenriquebarrios-pesquisaemcncerdesafiosparaaprximagerao-161121200234/85/Carlos-Henrique-Barrios-19-320.jpg)

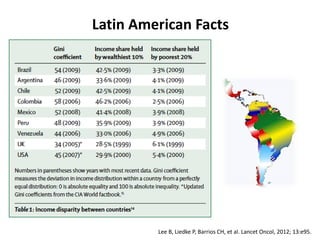
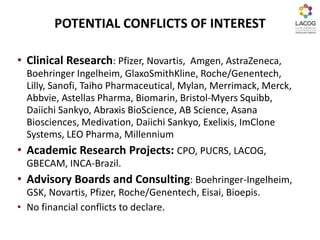
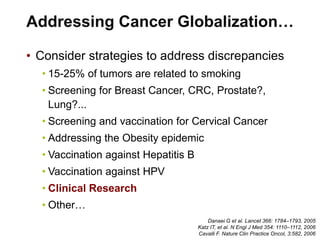
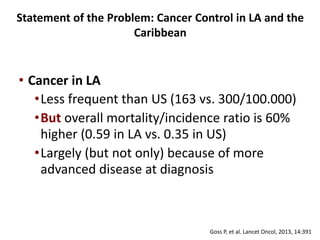
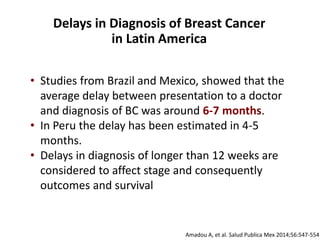
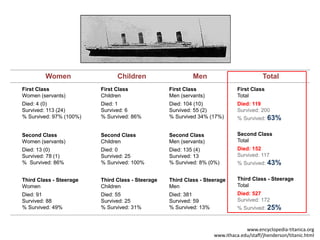
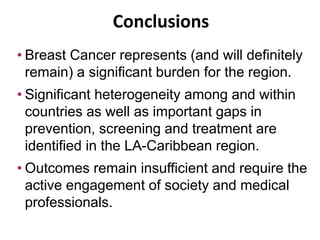
![Statement of the Problem: Cancer Control in LA and the
Caribbean
Projection of Cancer Incidence Burden 2012-2030
Bray F, Piñeros M. Cancer patterns, trends and projections in Latin America and the Caribbean: a global context. Salud Publica Mex 2016;58:104-117.
International Agency for Research on Cancer. WHO Cancer Mortality Database [accessed on November 17, 2015].
Available at: http://wwwdepiarc fr/WHOdb/WHOdb htm 2014.](https://image.slidesharecdn.com/carloshenriquebarrios-pesquisaemcncerdesafiosparaaprximagerao-161121200234/85/Carlos-Henrique-Barrios-43-320.jpg)
![Bray F, Piñeros M. Cancer patterns, trends and projections in Latin America and the Caribbean: a global context. Salud Publica Mex 2016;58:104-117.
International Agency for Research on Cancer. WHO Cancer Mortality Database [accessed on November 17, 2015].
Available at: http://wwwdepiarc fr/WHOdb/WHOdb htm 2014.
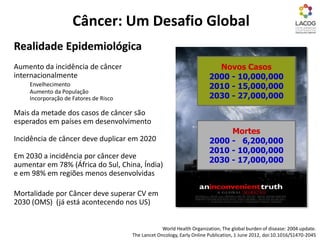
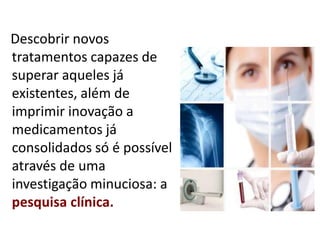
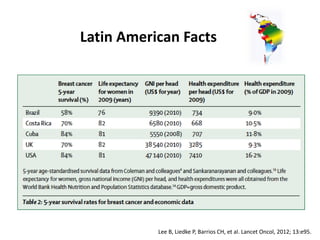
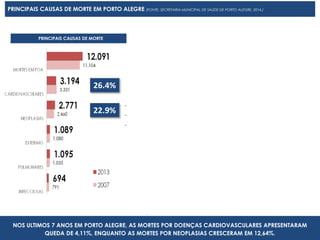
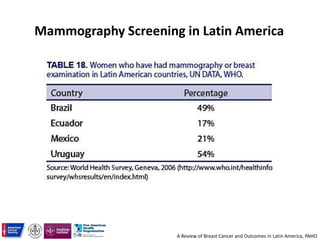
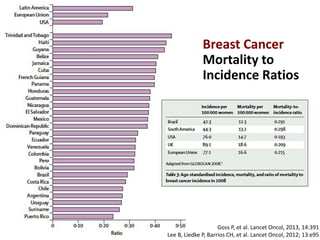
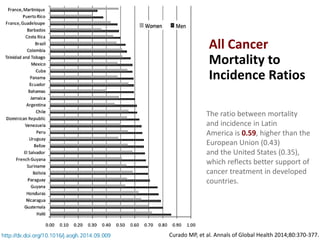
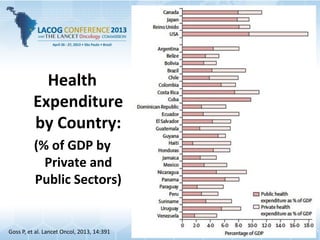
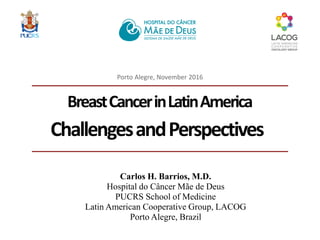
INCIDENCE MORTALITY
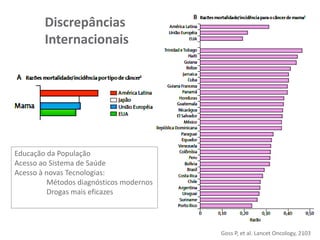
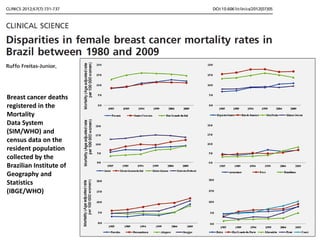
Despite the scarcity of cancer registries, we estimate that in most countries, breast cancer
incidence and mortality are increasing.
Trends in BC Incidence and Mortality
ASR per 100.000](https://image.slidesharecdn.com/carloshenriquebarrios-pesquisaemcncerdesafiosparaaprximagerao-161121200234/85/Carlos-Henrique-Barrios-53-320.jpg)

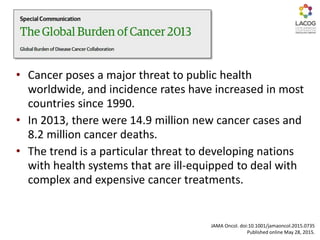
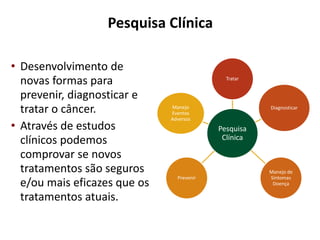
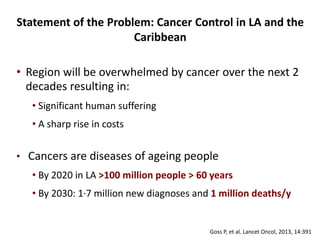
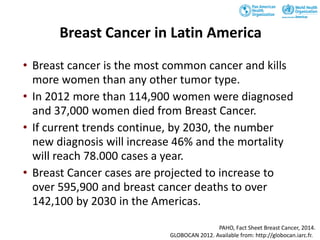
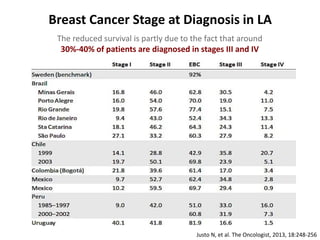
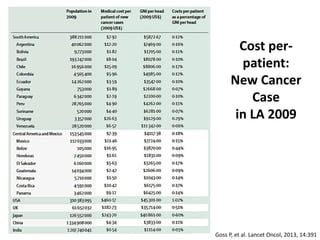
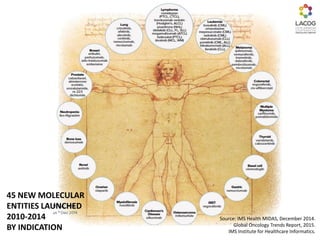
![Low and Middle Income Countries Spend
Less in Cancer Control
Medical Cancer Control spending per new cancer diagnosis
Numbers represent economic burden
per cancer patient in US$ (and as a
percentage of GDP/Capita)
Adapted from:
1. Economist Inteligence Unit. Breakaway: The global burden of cancer— challenges and opportunities [Internet]. 2009. Available de: http://www.livestrong.org/pdfs/GlobalEconomicImpact
2. United Nations. Per capita GNI at current prices [Internet]. 2012. Available de: http://data.un.org/Data.aspx?d=SNAAMA&f=grID%3A101%3BcurrID%3AUSD%3BpcFlag%3A1
3. United Nations. World Population Prospects, the 2010 Revision [Internet]. 2011. Available de: http://esa.un.org/wpp/index.htm
4. Lopes G, et al. Nature Rev Clin Oncol 2013.
Central America
and Mexico
$7.39](https://image.slidesharecdn.com/carloshenriquebarrios-pesquisaemcncerdesafiosparaaprximagerao-161121200234/85/Carlos-Henrique-Barrios-65-320.jpg)









































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)










