This is a an important topic and easily made to understand in cardiology basics to physiology and pathology and pharmacology..a detailed power point to understand easily.
من تنسونا الأرجوكم ,الهلي و لي جارية صدقة
دعائكم صالح
Please Grace us with your good prayers
معيوف يوسف
Youssef Maayouf
2.
Where does thesuperior vanae Cava drain
from ?
• Drains from heads and arms
3.
The tricuspid valveopens between which
champers?
• Right atrium and right ventricle
4.
What is thename of the muscles under the
valve?
• Papillary muscles
5.
Where does theinferior vanae Cava drain
from ?
• Drains from body and legs
6.
Where does theblood source to body and
legs come from ?
• From the descending aorta
7.
What is Pulsusparadoxus?
• Greater than the normal (10 mmHg) fall in systolic blood pressure
during inspiration
• Faint or absent pulse in inspiration
• It occurs with Severe asthma, cardiac tamponade
Which condition doespulsus alternans
associate with?
• It is Regular alternation of the force of the arterial pulse
• It’s associated with Severe LVF
11.
What is Bisferienspulse and Which condition
does it associate with?
•It’s 'Double pulse' - two systolic peaks
•Mixed aortic valve disease
•*HOCM may occasionally be associated with a bisferiens pulse
12.
What kind ofpulse is HOCM associated with ?
• 'Jerky' pulse (Like someone is Jerking off)
• “a rapid upstroke due to the vigorous contraction of the hypertrophic left
ventricle, as the volume of the left ventricle decreases there is a sudden
obstruction to the left ventricular outflow, outflow obstruction results in a rapid
fall in arterial pressure”
• HOCM may occasionally be associated with a bisferiens pulse
13.
What causes the1st
and 2nd
heart sounds ?
• The first heart sound (S1) is caused by closure of the mitral and
tricuspid valves.
• whilst the second heart sound (S2) is due to aortic and pulmonary
valve closure
14.
What are thecharacteristics that you might
hear with S1 ?
•Closure of mitral and tricuspid valves
•Soft if long PR or mitral regurgitation
•Loud in mitral stenosis
•Variable intensity in complete heart block
15.
What causes S2heart sound?
• caused by the closure of the aortic valve (A2) closely followed by that
of the pulmonary valve (P2)
16.
What are thecauses of Loud S2 heart sound?
• Hypertension: systemic (loud A2) or pulmonary (loud P2)
• Hyperdynamic states
• Atrial septal defect without pulmonary hypertension
17.
What are thecauses of soft S2 heart sound?
•Aortic stenosis
18.
What are thecauses of a fixed split S2 heart
sound?
Atrial septal defect
19.
What are thecauses of a widely split S2 heart
sound?
•Deep inspiration
•RBBB (Right bundle branch block)
•Pulmonary stenosis
•Severe mitral regurgitation
20.
What are theCauses of a reversed
(paradoxical) split S2 (P2 occurs before A2)?
•LBBB (|Left Bundle Branch Block)
•Severe aortic stenosis
•Right ventricular pacing
•WPW type B (causes early P2)
•Patent ductus arteriosus
21.
What causes theS3 heart sound?
•Caused by diastolic filling of the ventricle
•Considered normal if < 30 years old (may persist in women up to 50
years old)
•Heard in left ventricular failure, constrictive pericarditis
•Gallop rhythm (S3) is an early sign of LVF
22.
What causes theS4 heart sound?
•may be heard in aortic stenosis, HOCM, hypertension
•caused by atrial contraction against a stiff ventricle
•in HOCM a double apical impulse may be felt as a result of a palpable
S4
23.
What are theuses of measuring Jagular
Venus pulse?
• as well as providing information on right atrial pressure, the jugular
vein waveform may provide clues to underlying valvular disease.
A non-pulsatile JVP is seen in superior vena caval obstruction.
Kussmaul's sign describes a paradoxical rise in JVP during inspiration
• seen in constrictive pericarditis. Kussmaul's sign constrictive
pericarditis
24.
What is Kussmaul'ssign ?
Kussmaul's sign describes a paradoxical rise in JVP during inspiration
seen in constrictive pericarditis.
Kussmaul's sign constrictive pericarditis
25.
What is theJagular venous pulse A wave?
• a' wave = atrial contraction
• Large if high atrial pressure e.g. Tricuspid stenosis, pulmonary
stenosis, pulmonary hypertension
• Absent if in atrial fibrillation
26.
What are Jagularvenous pressure cannon A
waves?
•Caused by atrial contractions against a closed tricuspid valve
•Are seen in complete heart block, ventricular tachycardia/ectopics,
nodal rhythm, single chamber ventricular pacing
27.
What are thetypes of Cannon A waves and
what causes them?
• Cannon waves: May be subdivided into regular or intermittent
• Regular cannon waves
• Ventricular tachycardia (with 1:1 ventricular-atrial conduction)
• Atrio-ventricular nodal re-entry tachycardia (AVNRT)
• Irregular cannon waves
• Complete heart block
28.
What is theJagular venous pulse C wave?
• Closure of tricuspid valve
• Not normally visible
29.
What causes Jagularvenous pulse V waves?
•Giant v waves in tricuspid regurgitation
30.
What causes Jagularvenous pulse X descent?
• Fall in atrial pressure during ventricular systole
What are thephysiological changes in blood
pressure during exercise?
• Systolic increases, diastolic decreases
• Leads to increased pulse pressure (difference between systolic and
diastolic)
• In healthy young people the increase in MABP is only slight
33.
What are thephysiological changes in cardiac
output during exercise?
• increase in cardiac output may be 3-5 fold
• Results from venous constriction, vasodilation and increased myocardial
contractibility, as well as from the maintenance of right atrial pressure by
an increase in venous return
• Heart rate up to 3-fold
• Stroke volume up to 1.5-fold
34.
How to calculatethe left ventricular EF ?
• Left ventricular ejection fraction = (stroke volume / end diastolic LV
volume) * 100%
35.
What is thestroke volume ?
• Stroke volume = end diastolic LV volume - end systolic LV volume
36.
Left Bundle branchblock can be physiological,
T/F?
• False
• LBBB is always pathological
37.
What are theECG normal variants in an
athlete?
• Sinus bradycardia
• Junctional rhythm
• First degree heart block
• Wenckebach phenomenon
38.
What are theECG changes that may be seen
in hypothermia?
• Bradycardia
• 'J' wave (Very specific to hypothermia)- small hump at the end of the QRS
complex
• First degree heart block
• Long QT interval
• Atrial and ventricular arrhythmias
39.
When do weusually see J waves and delta
waves in ECG ?
• J waves are seen in hypothermia (Jwaves are positive deflections in
the terminal portion of the QRS complex and are highly sensitive and
specific for hypothermia)
• whilst delta waves are associated with WPW
40.
What are thefeatures of Digoxin with ECG ?
• Down-sloping ST depression ('reverse tick')
• Flattened/ inverted T waves
• Short QT interval
• Arrhythmias e.g. AV block, bradycardia
41.
What are thecauses of ST depression?
• Normal if upward sloping
• Ischemia
• Digoxin
• Hypokalemia
• Syndrome X
42.
ST depression withupward sloping is Normal,
T/F?
• True
• Normal if upward sloping
43.
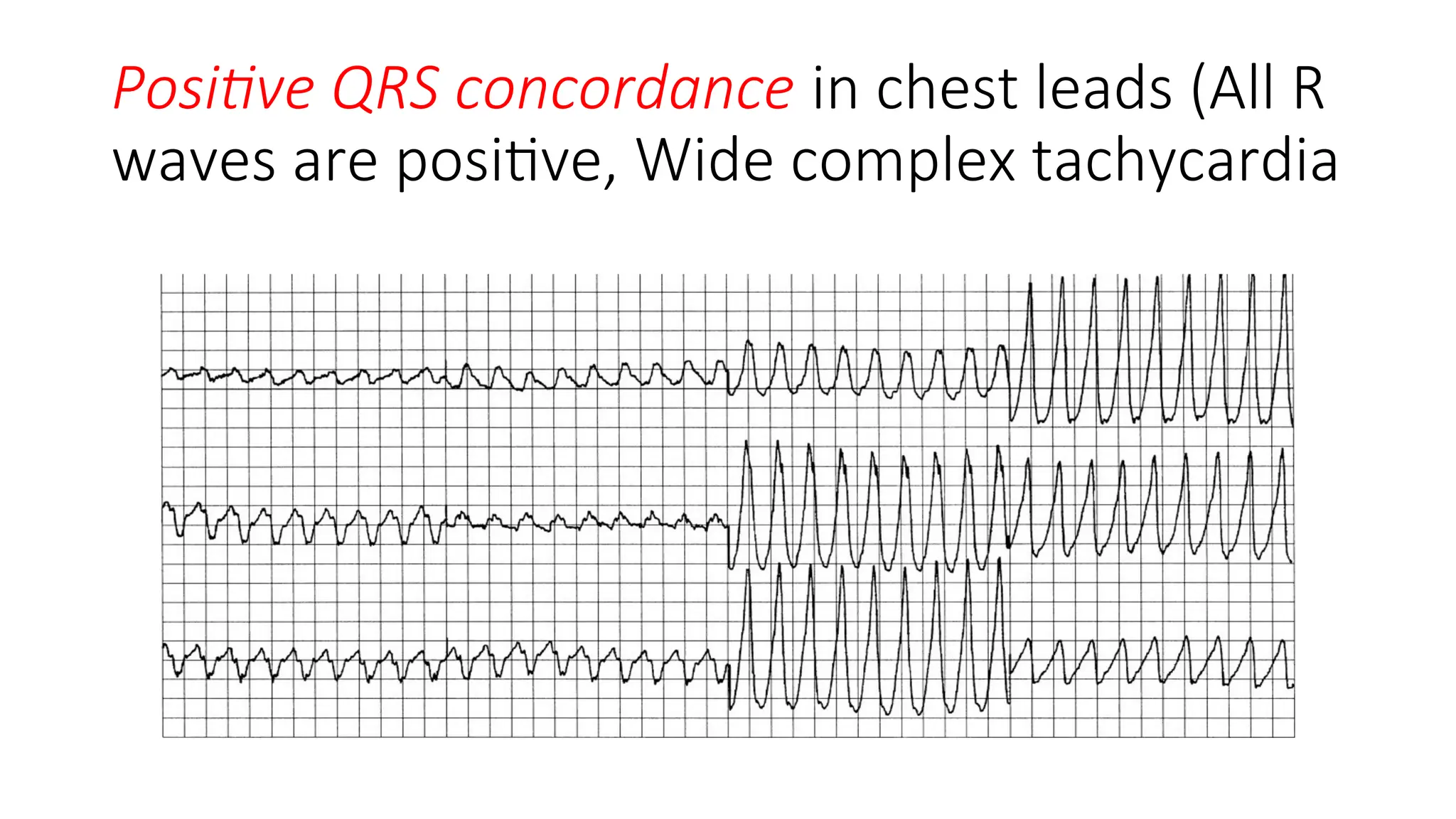
How to diagnoseLeft Bundle Branch Block?
• criteria to diagnose a left bundle branch block on ECG:
• Rhythm must be supraventricular in origin (P wave present)
• QRS duration >or= 120 ms (3 small squares)
• QS or rS complex in lead V1(note: r is small-not capital = small-not tall r in
ECG)
• RsR wave in lead V6 (slurred M-shaped QRS complexes in the lateral leads)
44.
What are thecauses of Left Bundle Branch
Block?
• Ischemic heart disease
• Hypertension
• Cardiomyopathy
• Idiopathic fibrosis
45.
How to diagnoseRight Bundle Branch Block?
• A classic right bundle branch block (RBBB) include: a prolonged QRS >
120 ms, an M-shaped QRS complexes in the right sided chest leads
and a slurred S wave in the lateral leads.
46.
What is ProlongedPR interval?
• PR interval is lengthened beyond 0.20 seconds (>5small squares)
• Also named: 1st degree heart block
47.
What are thecauses of prolonged PR
interval/first degree heart block?
• Idiopathic, Ischemic heart disease
• Digoxin toxicity
• Hypokalemia* (Hyperkalemia can rarely cause a prolonged PR interval)
• Rheumatic fever
• Aortic root pathology e.g. Abscess secondary to endocarditis
• Lyme disease
• Sarcoidosis
• Myotonic dystrophy
48.
A prolonged PRinterval may also be seen in
athletes, T/F?
• True
49.
WHY the confusionin right and left axis
deviation and rbb and left bbb and wpw ?
• Because we forget that the heart is 3 dimension, there is also
anterior (which makes the axis towards right and posterior which
makes the axis toward left)
• When the conduction is blocked in anterior area, it will make the
axis left (e.g. left anterior hemiblock causes left axis deviation)
• When the conduction is blocked posterior (left posterior hemiblock
causes right axis deviation)
50.
What are thecauses of Left Axis deviation in
ECG?
• Left anterior hemiblock
• Left bundle branch block
• Wolff-parkinson-white syndrome* - rightsided accessory pathway
• Hyperkalemia
• Congenital: ostium PRIMUM ASD, tricuspid atresia
• Minor LAD in obese people
51.
in the majorityof cases, or in a question without specification,
Wolff-Parkinson-White
syndrome is associated with left axis deviation, T/F?
• True
52.
What are theCauses of right axis deviation
(RAD)?
• Right ventricular hypertrophy
• Left posterior hemiblock
• Chronic lung disease
• Pulmonary embolism
• Ostium SECUNDUM ASD
• Wolff-parkinson-white syndrome* - leftsided accessory pathway
• Normal in infant < 1 years old
• Minor RAD in tall people
53.
What is Isolatedsystolic hypertension (ISH) ?
• Isolated systolic hypertension (ISH) is common in the elderly, affecting around 10%
of people older than 70 years old.
• The Systolic Hypertension in the Elderly Program (SHEP) back in 1991 established
that treating ISH decreases the risk of both strokes and ischemic heart disease.
• Drugs such as thiazides were recommended as first line agents. This approach is
not contraindicated by the 2006 NICE guidelines which recommend treating ISH in
the same stepwise fashion as standard hypertension
54.
What should beyour initial drug choice for
hypertension?
• Patients < 55-years-old: ACE inhibitor
• Patients > 55-years-old or of Afro-Caribbean origin: calcium channel
blocker or thiazide diuretic
• Older patients > 55 but with element of heart failure: ACE is better
55.
When treating hypertension, what is your
targeted blood pressure?
• The target blood pressure is 140/90 mmHg
56.
What should youdo if you’re not sure that
your patient has hypertension or not?
• When diagnosis of HTN is unclear, ambulatory 24H BP monitor may
be helpful
57.
Which life stylemodification has the biggest
impact on your patient hypertension?
• Weight reduction produces the greatest reduction in BP
• A 10 kg weight loss is expected to decrease the BP by 15–20 mmHg
• Salt restriction to less than 6g/day: 2–8mmHg
• Moderate alcohol consumption (less than 21 units a week for man and less than
14 units a week for women): 2.5–4 mmHg
58.
What would youdo next for your
hypertension patient if the first line single
drug that you prescribed didn’t work well?
• If this fails to control the blood pressure then use a combination of an
ACE inhibitor plus either a calcium channel blocker or thiazide diuretic
• If this still fails then a combination of an ACE inhibitor + calcium
channel blocker + thiazide diuretic should be used
59.
Should we prescribeBeta-Blockers to treat
hypertension?
• No
• Beta-blockers are less likely to prevent stroke + potential
impairment of glucose tolerance; this was demonstrated in the
Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure
Lowering Arm(ASCOT-BPLA)
60.
What are therenal causes of secondary
hypertension?
• Renal - accounts for 80% of secondary hypertension
• Glomerulonephritis
• Pyelonephritis
• Adult polycystic kidney disease
• Renal artery stenosis
61.
What are theEndocrine causes for secondary
hypertension?
• Cushing's syndrome
• Primary hyperaldosteronism including Conn's syndrome
• Liddle's syndrome
• Congenital adrenal hyperplasia (11- hydroxylase deficiency)
• Pheochromocytoma
• Acromegaly
62.
What are theNon-Renal, Non-Endocrine
causes of 2ndry hypertension?
• Pregnancy
• Coarctation of the aorta
• The combined oral contraceptive pill
• Steroids
• Mao inhibitors
63.
What are thenew antihypertensive drugs?
• Direct renin inhibitors
64.
What are thedirect renin inhibitors (new
antihypertensive drugs)?
• e.g. Aliskiren (branded as Rasilez)
• By inhibiting renin blocks the conversion of angiotensinogen to angiotensin I
• No trials have looked at mortality data yet. Trials have only investigated fall in blood
pressure.
• Initial trials suggest aliskiren decreases blood pressure to a similar extent as angiotensin
converting enzyme (ACE) inhibitors or angiotensin-II receptor antagonists
• Adverse effects were uncommon in trials although diarrhea was occasionally seen
• Only current role would seem to be in patients who are intolerant of more established
antihypertensive drugs
65.
What are thecentrally acting
antihypertensive drugs?
• Methyldopa: used in the management of hypertension during pregnancy
• Moxonidine: used in the management of essential hypertension when
conventional antihypertensives have failed to control blood pressure
• Clonidine: the antihypertensive effect is mediated through stimulating Alpha-2
adrenoceptors in the vasomotor center.
66.
What is theeffect of DM combined with
Hypertension?
• Hypertension and DM is an added cardiovascular risk factor for
diabetics and should therefore by actively looked for and treated.
• It is also a risk factor for the development of diabetic nephropathy.
67.
How to treatHypertension in a diabetic
patient?
• The blood pressure target for diabetics is 140/80 mmHg. If there is end-organ
damage the target is 130/80 mmHg
• ACE inhibitors are first-line*. Otherwise managed according to standard
NICE hypertension guidelines
• BNF advises to avoid the routine use of beta-blockers in uncomplicated
hypertension, particularly when given in combination with thiazides, as they may
cause insulin resistance, impair insulin secretion and alter the autonomic
response to hypoglycemia
68.
What is theeffect of ACE on a diabetic
patient?
• increase insulin sensitivity and can therefore theoretically cause
hypoglycemia - rarely clinically relevant
69.
What are thefeatures of Pericarditis?
• Chest pain: may be pleuritic. Is often relieved by sitting forwards
• Other symptoms include non-productive cough, dyspnea and flu-like
symptoms
• Pericardial rub
• Tachypnea
• Tachycardia
70.
What are thecauses of pericarditis?
• Viral infections (Coxsackie)
• TB
• Uremia (causes 'fibrinous' pericarditis)
• Trauma
• Post MI, Dressler's syndrome
• Connective tissue disease
• Hypothyroidism
71.
What are theECG changes with pericarditis?
• Widespread 'saddle-shaped' ST elevation
• PR depression
72.
What are thecauses of Myocarditis?
• Viral: coxsackie, HIV
• Bacteria: diphtheria, clostridia
• Spirochetes: Lyme disease
• Protozoa: Chagas' disease, toxoplasmosis
• Autoimmune
• Drugs
73.
What is thecommon presentation for
Myocarditis?
• Usually young patient with acute history
• Chest pain, Shortness of Breath
74.
What is thetreatment of pericarditis?
• First line is ibuprofen 800 mg four times per day
• Between 15% and 30% of patients with apparently idiopathic acute pericarditis
may have recurrent attacks and this is considered to be an autoimmune
phenomenon.
• Colchicine is useful both in acute episode and to prevent recurrence of
pericarditis.
• Prednisolone can be considered in patients who fail to respond to nonsteroidal
anti-inflammatory drug and colchicine therapy.
75.
What are therisk factors/associations for
developing infective endocarditis?
• Infective endocarditis: the strongest risk factor for developing
infective endocarditis is a previous episode of endocarditis. Other
factors include:
• Previously normal valves (50%, typically acute presentation)
• Rheumatic valve disease (30%)
• Prosthetic valves
• Congenital heart defects
• Intravenous drug users (IVDUS, e.g. Typically causing tricuspid lesion)
76.
What are theMostcommon cause of
endocarditis?
• Streptococcus viridans
• Staphylococcus epidermidis if < 2 months post valve surgery
77.
What are thecauses of infective
Endocarditis?
• Streptococcus viridans (most common cause - 40-50%) has good prognosis
• Staphylococcus epidermidis (especially prosthetic valves- 2 months)
• Staphylococcus aureus (especially acute presentation, IVDUS)
• Streptococcus bovis is associated with colorectal cancer
• Bacteroides fragilis endocarditis is very rare complication of colonic resection,
bacteria reaches heart via venous return, this is why it affects right > left side
Treat with Metronidazole
78.
What are thecauses for non-infective
endocarditis?
• Non-infective: systemic lupus erythematosus (Libman-Sacks),
malignancy, marantic endocarditis
79.
What are theculture-negative causes of
Infective endocarditis?
• Brucella
• Prior antibiotic therapy
• Coxiella burnetii
• HACEK: Hemophilus, Actinobacillus, Cardiobacterium, Eikenella, Kingella)
• Bartonella
80.
What is thecommonest organism to cause
infective endocarditis in a prosthetic valve
patient?
• Following prosthetic valve surgery Staphylococcus epidermidis is the most
common organism in the first 2 months and is usually the result of perioperative
contamination.
• After 2 months the spectrum of organisms which cause endocarditis return to
normal, except with a slight increase in Staph aureus infections
81.
What are thepoor prognostic factors for
infective endocarditis?
• Staph aureus infection (see below)
• Prosthetic valve (especially 'early', acquired during surgery)
• Culture negative endocarditis
• Low complement levels
82.
What are thedifferent mortality ratios for
different organisms causing infective
endocarditis?
• Staphylococci - 30%
• Bowel organisms - 15%
• Streptococci - 5%
83.
What is thegeneral scheme for diagnosing
infective endocarditis?
• Pathological criteria positive, or
• 2 major criteria, or
• 1 major and 3 minor criteria, or
• 5 minor criteria
84.
What are thepathological criteria for
diagnosing infective endocarditis?
• Positive histology or microbiology of pathological material obtained
at autopsy or cardiac surgery
• (valve tissue, vegetations, embolic fragments or intracardiac abscess
content)
85.
What are themajor criteria for diagnosing
infective endocarditis?
• Positive blood cultures
• Two positive blood cultures showing typical organisms consistent with infective endocarditis,
such as Streptococcus viridans and the HACEK group.
• Persistent bacteremia from two blood cultures taken > 12 hours apart or three or more
positive blood cultures where the pathogen is less specific such as Staph aureus and Staph
epidermidis.
• Positive serology for Coxiella burnetii, Bartonella species or Chlamydia psittaci.
• Positive molecular assays for specific gene targets
• 2. Evidence of endocardial involvement
• Positive echocardiogram (oscillating structures, abscess formation, new valvular regurgitation
or dehiscence of prosthetic valves), or
• New valvular regurgitation
86.
What are theminor criteria for diagnosing
infective endocarditis?
• Predisposing heart disease
• Microbiological evidence does not meet major criteria
• Fever > 38ºc
• Vascular phenomena: major emboli, splenomegaly, clubbing, splinter
hemorrhages, petechiae or purpura
• Immunological phenomena: glomerulonephritis, Osler's nodes, Roth spots (boat
shaped hemorrhages in retina)
• Elevated CRP or ESR
87.
What is thetreatment of Infective
endocarditis according to (British National
Formulary)?
• Initial blind therapy - flucloxacillin + gentamicin (benzylpenicillin + gentamicin if
symptoms less severe)
• Initial blind therapy if prosthetic valve is present or patient is penicillin allergic –
vancomycin + rifampicin + gentamicin
• Endocarditis caused by staphylococci - flucloxacillin (vancomycin +
rifampicin if penicillin allergic or MRSA)
• Endocarditis caused by streptococci benzylpenicillin + gentamicin
(vancomycin + gentamicin if penicillin allergic)
88.
What would yougive for Endocarditis in Native
valve and you do not know the organism?
• Amoxicillin + low-dose gentamicin
• If penicillin allergic, MRSA or severe sepsis
• vancomycin + low-dose gentamicin
89.
What would yougive for prosthetic valve
endocarditis caused by staphylococci?
• Flucloxacillin + rifampicin + low-dose gentamicin
• If penicillin allergic or MRSA
• vancomycin + rifampicin + low-dose gentamicin
• Initial blind therapy (Prosthetic valve but you do not know the organism)
• vancomycin + rifampicin + low-dose gentamicin
90.
What would yougive for Endocarditis caused
by fully-sensitive streptococci (e.g. viridans)?
• Benzylpenicillin
If penicillin allergic
vancomycin + low-dose gentamicin
91.
What would yougive for Native valve
endocarditis caused by staphylococci?
• Flucloxacillin
• If penicillin allergic or MRSA (vancomycin + rifampicin)
92.
What is thebest way to draw blood cultures
for patients with endocarditis?
• Microbiological diagnosis using blood cultures are essential for the diagnosis of
infective endocarditis, and ideally three sets of optimally filled blood cultures
should be taken from peripheral sites with greater than six hours between them
prior to antibiotics for patients with a subacute presentation.
• There is no evidence that blood cultures should be taken from different sites,
and taking blood cultures at different times is more important to pick up a
constant bacteraemia which is a feature of infective endocarditis.
93.
What are theindications for surgery for a
patient with infective endocarditis?
• Severe valvular incompetence (both native and prosthetic)
• Early prosthetic valve endocarditis
• Aortic abscess (often indicated by a lengthening PR interval)
• Infections resistant to antibiotics/fungal infections
• Cardiac failure refractory to standard medical treatment
• Recurrent emboli after antibiotic therapy
• HACK group, brucella, coxilla, pseudo- aeruginosa and vancomycin resistant
enterococci
94.
According to NICE2008, what are the
procedures that shouldn’t be given antibiotic
prophylaxis for endocarditis?
• NICE recommends the following procedures do not require
prophylaxis:
• Dental procedures
• Upper and lower gastrointestinal tract procedures
• Genitourinary tract; this includes urological, gynecological and obstetric
procedures and childbirth
• Upper and lower respiratory tract; this includes ear, nose and throat
procedures and bronchoscopy
95.
According to NICE2008, what are the
procedures that should be given antibiotic
prophylaxis for endocarditis?
• Any episodes of infection in people at risk of infective endocarditis should be
investigated and treated promptly to decrease the risk of endocarditis
developing
• If a person at risk of infective endocarditis is receiving antimicrobial therapy
because they are undergoing a gastrointestinal or genitourinary procedure at a
site where there is a suspected infection they should be given an antibiotic that
covers organisms that cause infective endocarditis
96.
What are thedrugs that have been shown to improve
mortality in patients with chronic heart failure?
• ACE inhibitors (SAVE, SOLVD, CONSENSUS)
• Spironolactone (RALES)
• Beta-blockers (CIBIS) (In case of fluid overload they can be stopped temporarily while
introducing spironolactone)
• Hydralazine with nitrates (VHEFT-1)
97.
Which Beta blockersare allowed to be used
for Heart Failure?
• Bisoprolol, carvedilol, nebivolol and metoprolol are the only
evidence-based cardioselective beta blockers for heart failure
98.
Whilst spironolactone hasbeen shown to improve prognosis in patients
with chronic heart failure, no long-term reduction in mortality has been
demonstrated for loop diuretics such as furosemide, T/F?
• True
• Whilst spironolactone has been shown to improve prognosis in
patients with chronic heart failure, no long-term reduction in
mortality has been demonstrated for loop diuretics such as
furosemide.
• NICE guidelines recommend the introduction of an ACE inhibitor prior
to a Beta-blocker in patients with chronic heart failure.
99.
What is Eplerenone?
•Eplerenone (INN) is a steroidal antimineralocorticoid used as an adjunct in the
management of chronic heart failure. It is similar to the diuretic spironolactone,
though it is much more selective for the mineralocorticoid receptor in
comparison
• Eplenerone is thus preferred to spironolactone to treat heart failure in
patients with recent myocardial infarctions.
100.
What are theNICE 2003 guidelines for
treating chronic heart failure?
• All patients should be given an ACE inhibitor unless contradictions exist
• Once an ACE inhibitor has been introduced a Beta-blocker should be started
regardless of whether the patient is still symptomatic
• Offer annual influenza vaccine
• Offer pneumococcal vaccine
101.
Should you givedigoxin to a patient with
heart failure ?
• Digoxin has also not been proven to decrease mortality in patients with heart
failure.
• It may however improve symptoms due to its inotropic properties.
• Digoxin is strongly indicated if there is coexistent atrial fibrillation
102.
A patient withheart failure resulting from
Amyloidosis (History of RF) who suffers from
Atrial fibrillation, should you give digoxin?
• No
• Digoxin is contraindicated in amyloid patients as patients are
extremely sensitive to it. This is possibly due to digoxin binding in the
amyloid fibrils.
103.
A patient withheart failure that’s refractory to
medications and in his ECG you find bundle branch
block, what could help improve his symptoms?
• Bundle branch blocks or intraventricular conduction delay (IVCD) cause ventricular dyssynchrony
and reduces the cardiac contractile function. This leads to worsening of heart failure symptoms.
Such patients have poorer exercise tolerance and worse prognosis compared to patients with
normal sinus rhythm.
• Cardiac resynchronisation therapy by biventricular pacing improves left ventricular
contractile function in patients with left bundle branch block (LBBB) or IVCD, and thus improves
symptoms. National Institute for Health and Care Excellence (NICE) guidelines recommend that
cardiac resynchronisation therapy should be considered in patients with left ventricular ejection
fraction less than 35%, drug refractory symptoms and QRS duration of greater than 120 ms.
104.
A patient withheart failure that’s refractory to
medications and not a candidate for heart
transplantation what could help improve his symptoms?
• Left ventricular assist device
• Data suggest that highly selected patients with refractory heart failure may be candidates for
implantation of a LVAD as a permanent or destination therapy.
• These are patients who are not expected to recover from heart failure and who are unsuitable for
transplant due to age or co-morbidities. Survival with LVADs is currently about 50% at 1 year.
105.
What is theThe New York Heart Association
(NYHA) classification for heart failure, class 1 and
2?
• NYHA Class I
• No symptoms
• No limitation: ordinary physical exercise does not cause undue fatigue,
dyspnea or palpitations
• NYHA Class II
• Mild symptoms
• Slight limitation of physical activity: comfortable at rest but ordinary activity
results in fatigue,palpitations or dyspnea
106.
What is theThe New York Heart Association
(NYHA) classification for heart failure, class 3 and
4?
• NYHA Class III
• Moderate symptoms
• Marked limitation of physical activity: comfortable at rest but less than
ordinary activity results in symptoms
• NYHA Class IV
• Severe symptoms
• Unable to carry out any physical activity without discomfort: symptoms of
heart failure are present even at rest with discomfort with any physical
activity
107.
According to AmericanHeart Association Advanced
Cardiac Life Support guidelines, what is the initial
treatment of acute pulmonary edema?
• High-flow oxygen
• Furosemide 0.5-1 mg/kg IV
• Morphine 2-4 mg IV
• Sublingual nitroglycerine (GTN).
108.
According to AmericanHeart Association Advanced Cardiac
Life Support guidelines, what should you do after the initial
treatment of acute pulmonary edema?
• Steps then are dictated by the systolic BP after initial treatment:
• If the BP is >100 mmHg, start IV nitroglycerine 10-20 μg/min
• BP of 70-100 mmHg, with no shock start IV dobutamine 2-20 μg/min
• If the BP is 70-100 mmHg with shock, start IV dopamine 5-15 μg/min
• If the BP is < 70 mmHg with shock, start IV noradrenaline 0.5-30 μg/min.
109.
Why is dopaminemore safe than
dobutamine?
• dopamine acts primarily as a beta-1 agonist, leading to improved
cardiac output because of increased cardiac contractility and stroke
volume.
• Dobutamine is not selective for the beta-1 receptor and may be
associated with increased risk of myocardial ischaemia and
tachyarrhythmias versus dopamine.
110.
What are theepidemics of diastolic heart
failure?
• 1/3 of heart failure is diastolic (normal Left Ventricular Systolic
Function-LVSF)
• Mortality in Diastolic HF is 5-8% (lower than Systolic HF: 10-15%)
111.
How to diagnoseDiastolic heart failure?
• Echo is the golden diagnostic tool
• CXR and ECG cannot differentiate Diastolic vs. Systolic HF.
112.
How to managediastolic heart failure?
• Initially, reduction of pulmonary venous pressure (PVP) and
congestion, using diuretics
• ARBs are superior to ACE inhibitors
113.
ARBs are superiorto ACE inhibitors in treating
diastolic heart failure, T/F?
• True
114.
What are thefeatures of cardiac tamponade?
• Becks triad, consisting of systemic hypotension, prominent neck veins and quiet heart
sounds
• Raised JVP, with an absent Y descent - this is due to the limited right ventricular filling
• Tachycardia
• Hypotension
• Muffled heart sounds
• Pulsus paradoxus (which occurs also in Asthma)
• Kussmaul's sign (much debate about this) (more in constrictive pericarditis)
• ECG: electrical alternans
115.
How to differentiatebetween cardiac
tamponade and constrictive pericarditis?
• Cardiac tamponade Constrictive pericarditis
• JVP Absent Y descent X + Y present
• Pulsus paradoxus Present Absent
• Kussmaul's sign Rare Present
• Characteristic features Pericardial calcification on CXR
116.
What is anX-ray characteristic feature for
constrictive pericarditis?
• Pericardial calcification on CXR
117.
What is themost common cause of
constrictive pericarditis worldwide?
• Tuberculous pericarditis is the commonest cause of constrictive
pericarditis worldwide
118.
A commonly usedmnemonic to remember the the features
and the absent Y descent in cardiac tamponade is TAMponade
=TAMpaX, T/F?
• True
119.
What are theDLVA rules for cardiology
conditions that restricts from driving?
• Angioplasty (elective) - 1 week off driving
• CABG - 4 weeks off driving
• Acute coronary syndrome- 4 weeks off driving, 1 week if successfully treated by angioplasty
• Angina - driving must cease if symptoms occur at rest/at the wheel
• Pacemaker insertion - 1 week off driving
• Implantable cardioverter-defibrillator: if implanted for sustained ventricular arrhythmia: cease driving for 6 months. If
implanted prophylatically then cease driving for 1 month
• Successful catheter ablation - 2 days off driving
• Aortic aneurysm > 6cm - notify DVLA. Licensing will be permitted subject to annual review.
• An aortic diameter of 6.5 cm or more disqualifies patients from driving
• Heart transplant: DVLA do not need to be notified
120.
What are thedifferent types of nuclear
imaging of the heart?
• These techniques use radiotracers which are extracted by normal myocardium,
Examples include:
• Thallium
• 'MIBI' or (SPECT) scans: Cardiac Single Photon Emission Computed Tomography
uses Technetium (99mTc) sestamibi, a coordination complex of the radioisotope
technetium-99m with the ligand methoxyisobutylisonitrile (MIBI).
• Positron Emission Tomography (PET) scans: Fluordeoxyglucose (FDG) is used.
121.
What do youknow about SPECT and cardiac
PET as a nuclear imaging tools for the heart?
• The primary role of SPECT is to assess myocardial perfusion and myocardial
viability. Two sets of images are usually acquired.
• First the myocardium at rest followed by images of the myocardium during stress
(either exercise or following adenosine / dipyridamole). By comparing the rest
with stress images any areas of ischemia can be classified as reversible or fixed
(e.g. following a myocardial infarction).
• Cardiac PET is predominately a research tool at the current time
122.
What is Mugascan?
• Multi Gated Acquisition Scan, also known as radionuclide angiography
• Radionuclide (technetium-99m) is injected intravenously
• The patient is placed under a gamma camera
• May be performed as a stress test
• Can accurately measure left ventricular ejection fraction. Typically used
before and after cardiotoxic drugs are used
123.
What do youknow about Cardiac computed
tomography?
• Cardiac Computed Tomography (CT): useful for assessing suspected IHD, using
two main methods:
• Calcium score: there is known to be a correlation between the amount of
atherosclerotic plaque calcium and the risk of future ischemic events. Cardiac CT
can quantify the amount of calcium producing a 'calcium score'
• Contrast enhanced CT: allows visualization of the coronary artery lumen
• If these two techniques are combined cardiac CT has a very high negative
predictive value for ischemic heart disease.
124.
What do youknow about Cardiac MRI?
• Cardiac MRI: (commonly termed CMR) has become the gold standard for
providing structural images of the heart.
• It is particularly useful when assessing congenital heart disease, determining
right and left ventricular mass and differentiating forms of cardiomyopathy.
Myocardial perfusion can also be assessed following the administration of
gadolinium.
• Currently CMR provides limited data on the extent of coronary artery disease.
125.
Can cardiac MRIbe used to asses myocardial
perfusion?
• Yes
• Myocardial perfusion can also be assessed following the
administration of gadolinium.
126.
Which patient shouldn’thave exercise ECG as
a method for evaluation of cardiac perfusion?
• It is USELESS in patients with:
• Conduction abnormalities
• resting (ECG) abnormalities like ST segment depression of >1mm
• WPW
• Digoxin
• Ventricular paced rhythm
• In such patients myocardial perfusion imaging is the preferred modality for
evaluation of CAD.
127.
What are theNICE guidelines for immediate
management for suspected acute coronary
syndrome?
• Glyceryl trinitrate
• Aspirin 300mg. NICE do not recommend giving other antiplatelet agents (i.e.
Clopidogrel) outside of hospital
• Do not routinely give oxygen, only give if sats < 94%*
• Perform an ECG as soon as possible but do not delay transfer to hospital. A
normal ECG does not exclude ACS
128.
A normal ECGexcludes acute coronary
syndrome, T/F?
• False
129.
According to NICEguidelines, when should
you refer a patient that you suspect with
acute cardiac syndrome?
• Current chest pain or chest pain in the last 12 hours with an abnormal ECG:
emergency admission
• Chest pain 12-72 hours ago: refer to hospital the same-day for assessment
• Chest pain > 72 hours ago: perform full assessment with ECG and troponin
measurement before deciding upon further action
130.
According to NICEguidelines , how should oxygen
treatment be given in a case of acute coronary
syndrome?
• Do not routinely administer oxygen, but monitor oxygen saturation using pulse
oximetry as soon as possible, ideally before hospital admission. Only offer
supplemental oxygen to:
• People with oxygen saturation (SpO2) < 94% who are not at risk of hypercapnic
respiratory failure, aiming for SpO2 of 94-98%
• People with chronic obstructive pulmonary disease who are at risk of hypercapnic
respiratory failure, to achieve a target SpO2 of 88-92% until blood gas analysis is
available.
131.
What are theNICE guidelines for assessing
patient presenting with stable chest pain ?
• They suggest an approach where the risk of a patient having coronary artery disease (CAD) is
calculated based on their symptoms (whether they have typical angina, atypical angina or non-anginal
chest pain), age, gender and risk factors.
• NICE define anginal pain as the following:
• Constricting discomfort in the front of the chest, neck, shoulders, jaw or arms
• Precipitated by physical exertion
• Relieved by rest or GTN in about 5 minutes
• Patients with all 3 features have typical angina
• Patients with 2 of the above features have atypical angina
• Patients with 1 or none of the above features have non-anginal chest pain
132.
What should youdo next for a patient that
you diagnosed with typical anginal
symptoms?
• If patients have typical anginal symptoms and a risk of CAD is greater than 90%
then no further diagnostic testing is required.
• It should be noted that all men over the age of 70 years who have typical anginal
symptoms fall into this category.
133.
For patients withan estimated risk of 10-90% (less than
90% risk, not 3 categories on the NICE guidelines) after
diagnosing anginal pain what should be the following
investigations?
• 61-90% risk :Coronary angiography
• 30-60% risk: Functional imaging, for example:
• Myocardial perfusion scan with SPECT
• Stress echocardiography
• First-pass contrast-enhanced magnetic resonance (MR) perfusion
• MR imaging for stress-induced wall motion abnormalities.
• 10-29% risk: CT calcium scoring
134.
According to theguidelines, do we use ECG stress test
as a diagnostic test to assess cardiac perfusion in a
patient presenting with symptoms of stable angina?
• No
135.
What is stableAngina?
• It’s when you have a patient presenting with chest pain but when you
assess his enzymes (Troponin) you find no cardiac damage, so he
suffers from ischemia with effort sometimes but didn’t cause a
cardiac damage
136.
What is themanagement of stable angina?
• the management of stable angina comprises lifestyle changes,
medication, percutaneous coronary intervention and surgery.
137.
What is themanagement of stable angina?
• NICE recommends the routine prescription of a short acting nitrate for stable
angina, followed by either a beta blocker or calcium channel blocker as first line
therapy with insufficient symptomatic control.
• Next, NICE recommends combining both beta blockers and calcium channel blockers.
• If previous failed, NICE recommends addition of either ranolazine, nicorandil,
ivrabradine or a long acting nitrate
• Patients requiring more than 2 anti-anginals should be considered for reperfusion
therapies1, with addition of a third drug only if the patient is not a candidate for PCI
or CABG.
138.
What are theguidelines for treatment of
stable angina according to NICE?
• In good exercise tolerance, consider medical therapy before angiography (Beta-
blocker is the most important)
• If pain is worsening, no need for exercise test, directly do angiography (Cath)
139.
What is thedrug management of stable
angina?
• All patients should receive aspirin and a statin in the absence of any
contraindication
• Sublingual glyceryl trinitrate to abort angina attacks
• Beta-blocker is the preferred initial treatment. If there is a poor response to initial
treatment then the Beta-blocker should be to the maximum tolerated dose (e.g.
atenolol 100mg od)
• Again, there are no clear guidelines on the next step treatment. CKS advise
adding a long-acting dihydropyridine (e.g. nifedipine, amlodepine, felodipine)
although other options include isosorbide mononitrate and nicorandil
140.
What should yougive to a stable angina
patient that can’t take a beta blocker?
• For patients unable to take a Beta -blocker there is no clear guidelines on the
best alternative.
• Options include a rate-limiting calcium-channel blocker (verapamil or diltiazem);
a long-acting dihydropyridine calcium-channel blocker (e.g. modifiedrelease
nifedipine); a nitrate; or a potassium-channel activator
141.
What is thetreatment of Prinzmetal angina?
• Prinzmetal angina - treatment = dihydropyridine calcium channel
blocker (depine family; amlodepine)
142.
How should youmanage nitrate tolerance for
patients treated from stable angina?
• Many patients who take nitrates develop tolerance and experience efficacy
• BNF advises that patients who develop tolerance should take the second dose of
isosorbide mononitrate after 8 hours, rather than after 12 hours.
• This allows blood-nitrate levels to fall for 4 hours and maintains effectiveness
• This effect is not seen in patients who take modified release isosorbide
mononitrate
143.
What do youknow about
Ivabradine(procoralan) in treatment of stable
angina?
• A new class of anti-anginal drug which works by reducing the heart rate
• Acts on the If ('funny') ion current which is highly expressed in the sinoatrial node,
reducing cardiac pacemaker activity
• Adverse effects: visual effects, particular luminous phenomena, are common.
Bradycardia, due to the mechanism of action, may also be seen
• There is no evidence currently of superiority over existing treatments of stable
angina
144.
What are theguidelines for treatment of
acute coronary syndrome ?
• The management of non-ST elevation acute coronary syndrome is based upon
the calculation of a risk score, for example TIMI (Thrombolysis In Myocardial
Infarction)
• All patients should receive
• - Aspirin 300mg
• - Nitrates or morphine to relieve chest pain if required
• Clopidogrel 300mg and low molecular weight heparin (principally enoxaparin)
should also be added to higher risk patients
145.
Should you giveoxygen to all patient with
acute coronary syndrome?
• Whilst it is common that non-hypoxic patients receive oxygen therapy there is
little evidence to support this approach.
• The 2008 British Thoracic Society oxygen therapy guidelines advise NOT GIVING
OXYGEN UNLESS THE PATIENT IS HYPOXIC.
146.
What do youknow about the Antithrompin treatment
that should be offered to acute coronary syndrome
patient?
• It depends on what you are going to do next to this patient:
• Fondaparinux should be offered to patients who are not at a high risk of bleeding
and who are not having angiography within the next 24 hours.
• If angiography is likely within 24 hours or a patient’s creatinine is > 265 μmol/l
unfractionated heparin (or Low molecular weight heparin ) should be given.
• Clopidogrel 300mg should be given to patients with a predicted 6 month
mortality of more than 1.5% or patients who may undergo percutaneous
coronary intervention within 24 hours of admission to hospital. Clopidogrel
should be continued for 12 months.
147.
What do youknow about the Antithrompin treatment
that should be offered to acute coronary syndrome
patient?
• It depends on what you are going to do next to this patient:
• If angiography is likely within 24 hours:
• unfractionated heparin (or Low molecular weight heparin ) should be given.
• Clopidogrel 300mg
• If no angiography is likely within 24 hours:
• Fondaparinux
• If angiography is likely within 96 hours (and a high risk patient)
• Intravenous glycoprotein IIb/IIIa receptor antagonists (eptifibatide or tirofiban)
148.
What do youknow about the Clopidogrel
(Plavix®) Interactions?
• Concurrent use of proton pump inhibitors (PPIs) may make
clopidogrel less effective (MHRA July 2009)
• This advice was updated by the MHRA in April 2010, evidence seems
inconsistent but omeprazole and esomeprazole still cause for concern.
• Other PPIs such as lansoprazole should be OK
149.
What do youknow about the use of Intravenous glycoprotein
IIb/IIIa receptor antagonists for treatment of patient with
acute coronary syndrome?
• Intravenous glycoprotein IIb/IIIa receptor antagonists (eptifibatide or tirofiban)
should be given to patients who have an intermediate or higher risk of adverse
cardiovascular events (predicted 6-month mortality above 3.0%), and who are
scheduled to undergo angiography within 96 hours of hospital admission.
150.
When should wedo coronary angiography for a
patient with acute coronary syndrome?
• Coronary angiography should be considered within 96 hours of first admission to
hospital to patients who have a predicted 6-month mortality above 3.0%.
• It should also be performed as soon as possible in patients who are clinically
unstable.
151.
What is theaction Aspirin of as a drug used for
management of Acute coronary syndrome?
• Antiplatelet - inhibits the production of thromboxane A2
152.
What is theaction of Clopidogrel as a drug used
for management of Acute coronary syndrome?
• Antiplatelet - inhibits ADP binding to its platelet receptor
153.
What is theaction of Enoxaparin as a drug used
for management of Acute coronary syndrome?
• Activates antithrombin III, which in turn potentiates the inhibition of
coagulation factors Xa
154.
What is theaction of Fondaparinux as a drug used
for management of Acute coronary syndrome?
• Activates antithrombin III, which in turn potentiates the inhibition of
coagulation factors Xa
155.
What is theaction of Bivalirudin as a drug used for
management of Acute coronary syndrome?
• Reversible direct thrombin inhibitor
156.
What are thepoor prognostic factors for
patient with Acute coronary syndrome?
• Age
• Development (or history) of heart failure, Killip class*
• Peripheral vascular disease
• Decreased systolic blood pressure
• Initial increased serum creatinine concentration
• Elevated initial cardiac markers
• Cardiac arrest on admission
• ST segment deviation
157.
What is Killipclass used to evaluate prognosis in patient
with acute cardiac symptoms using evidence of heart
failure?
• Killip class - system used to stratify risk post myocardial infarction
• Killip class Features 30 day mortality
• I No clinical signs heart failure 6%
• II Lung crackles, S3 17%
• III Frank pulmonary edema 38%
• IV Cardiogenic shock 81%
158.
What do youknow about the coronary
circulation of the heart?
• Coronary Circulation (arterial supply of the heart)
• Posterior aortic or coronary sinus gives left coronary artery (LCA)
• Anterior aortic or coronary sinus gives right coronary artery (RCA)
• LCA (Left Main, LM) gives LAD + circumflex
• RCA gives posterior descending
• RCA supplies SA node in 60%, AV node in 90%
159.
Which coronary arteryis blocked when you
see ECG changes in V1-V4?
• Anteroseptal
• Left anterior descending
160.
Which coronary arteryis blocked when you
see ECG changes in II, III, aVF ?
• Inferior part of the heart
• Right coronary
161.
Which coronary arteryis blocked when you
see ECG changes in V4-6, I, aVL ?
• Anterolateral
• Left anterior descending or left circumflex
162.
Which coronary arteryis blocked when you
see ECG changes in I, aVL +/- V5-6 ?
• Lateral
• Left circumflex
163.
Which coronary arteryis blocked when you
see ECG changes in Tall R waves V1-2 ?
• Posterior
• Usually left circumflex, also right coronary
164.
Which drugs shouldall patients with
myocardial infarction receive?
• All patients should be offered the following drugs:
• ACE inhibitor
• Beta-blocker
• Aspirin
• Statin
165.
How is bloodsupply to the heart drained?
• Venous drainage of the heart: coronary sinus drains into the right
atrium
166.
What is therole of clopidogril(plavix) in
treating myocardial infarction?
• After an ST-segment-elevation MI, patients treated with a combination of aspirin
and clopidogrel during the first 24 hours after the MI should continue this
treatment for at least 4 wk
• (NSTEMI): following the 2010 NICE unstable angina and NSTEMI guidelines
clopidogrel should be given for the first 12 months if the 6 month mortality risk is >
1.5%
• Improves prognosis post MI
• Side effect: < 1% TTP usually 2 weeks after commencing the drug.
167.
What is therole of aldosterone antagonists
for treating MI?
• Patients who have had an acute MI and who have symptoms and/or
signs of heart failure and left ventricular systolic dysfunction,
treatment with an aldosterone antagonist licensed for post MI
treatment should be initiated within 3-14 days of the MI,
• preferably after ACE inhibitor therapy
168.
What are thecontraindications of
Thrompolytic therapy?
• Active internal bleeding
• Recent hemorrhage, trauma or surgery (including dental extraction)
• Coagulation and bleeding disorders
• Intracranial neoplasm
• Stroke < 2 months
• Aortic dissection
• Recent head injury
• Pregnancy
• Severe hypertension
169.
What is Dessler’ssyndrome?
• Dressler's syndrome is a secondary form of pericarditis that occurs in the setting
of injury to the heart or the pericardium (the outer lining of the heart).
• It consists of a triad of features, fever, pleuritic pain and pericardial effusion.
170.
What are thefeatures of Dessler’s syndrome?
• Malaise, fever, pericardial pain
• Elevated erythrocyte count
• Sometimes may also have pleuritis and pneumonitis.
171.
What are thecauses of Dessler’s
syndrome(pericarditis following
endocarditis)?
• It has been postulated that the syndrome results from release of cardiac antigens
which then stimulate antibody production.
• The immune complexes are then deposited in the pericardium, pleura and lung.
• There may be accompanying pleural and pericardial effusion and therefore
echocardiography should be done.
172.
What is thetreatment of Dessler’s
syndrome?
• Treatment involves aspirin and analgesics.
• Corticosteroids and non-steroidal anti-inflammatory agents are best avoided in
the first 4 weeks after MI as they delay myocardial healing.
• Aspirin in large doses is effective.
• Recurrences can occur, and in such cases colchicine is helpful.
173.
What is themanagement that should be
given to each patient with ST Elevation
Myocardial Infarction (STEMI)?
• Aspirin
• Clopidogrel: the two major studies (clarity and commit) both confirmed benefit
but used different loading doses (300mg and 75mg respectively)
• Low molecular weight heparin
174.
What is thegold standard treatment for ST
Elevation Myocardial Infarction (STEMI)?
• Primary percutaneous coronary intervention (PCI) has emerged as the gold-
standard treatment for STEMI but is not available in all centers.
• Thrombolysis should be performed in patients without access to primary PCI
175.
What is thedifference between Tissue
plasminogen activator (TPA), streptokinase
and Tenecteplase as thrompolysis treatment?
• Tissue plasminogen activator (TPA) has been shown to offer clear
mortality benefits over streptokinase
• Tenecteplase is easier to administer and has been shown to have non-
inferior efficacy to alteplase with a similar adverse effect profile
176.
What are theguidelines when given
thrompolysis treatment?
• An ECG should be performed 90 minutes following thrombolysis to assess
whether there has been a greater than 50% resolution in the ST elevation
• If there has not been adequate resolution then rescue PCI is superior to repeat
thrombolysis
• For patients successfully treated with thrombolysis PCI has been shown to be
beneficial.
• The optimal timing of this is still under investigation
177.
What is PercutaneousCoronary Intervention
(PCI)?
• Percutaneous Coronary Intervention (PCI) is a technique used to restore
myocardial perfusion in patients with ischemic heart disease, both in patients with
stable angina and acute coronary syndromes.
• Stents are implanted in around 95% of patients - it is now rare for just balloon
angioplasty to be performed.
• Before PCI, visualization of the coronaries is needed using diagnostic angiography.
178.
What are thecomplications of coronary
angioplasty?
• Vascular complications: the most common complication overall is hemorrhage from
access (right femoral artery mostly then right radial artery), much less common is rupture
of coronary artery during revascularization or rupture of any artery from access to target
artery
• Contrast Induced Nephropathy (CIN), higher incidence in diabetic patients and patients
known to have renal dysfunction (prevented by good hydration)
• Cholesterol embolisation
• Arrhythmias (include arrest, ventricular and supraventricular) especially in primary
intervention (in case of acute MI)
• Reaction to contrast
179.
What happens tothe stent after insertion in
coronary vessels?
• Following stent insertion migration and proliferation of smooth muscle cells and
fibroblasts occur to the treated segment.
• The stent struts eventually become covered by endothelium.
• Until this happens there is risk of platelet aggregation leading to thrombosis.
180.
What are thecomplications of stenting a
coronary vessel?
• Two main complications may occur due to stenting:
• Stent thrombosis: due to platelet aggregation as above. Occurs in 1-2% of
patients, most commonly in the first month. Usually presents with acute
myocardial infarction
• Restenosis: due to excessive tissue proliferation around stent. Occurs in around
5-20% of, patients, most commonly in the first 3-6 months. Usually presents with
the recurrence of angina symptoms. Risk factors include diabetes, renal
impairment and stents in venous bypass grafts
181.
What are therisk factors of restenosis after
stenting of a coronary?
• 5-20% of, patients ,Risk factors include diabetes, renal impairment
and stents in venous bypass grafts
182.
What are thetypes of stents?
• Bare-metal stent (BMS)
• Drug-eluting stents (DES): stent coated with paclitaxel or rapamycin which
inhibit local tissue growth. Whilst this decreases restenosis rates the stent
thrombosis rates are as the process of stent endothelisation is slowed
183.
What are therisk of restenosis in Bare metal
stent in a Type2 DM patient?
• BMS in T2DM: restenosis risk in 6 months is 40-50%
184.
How to decreasethe rate of thrombosis after
coronary stenting?
• Following insertion the most important factor in preventing stent
thrombosis is antiplatelet therapy.
• Aspirin should be continued indefinitely.
• The length of clopidogrel treatment depends on the type of stent,
reason for insertion and consultant preference.
185.
What is clopidogriland what is the action?
• Clopidogrel is a pro-drug whose action may be related to adenosine diphosphate (ADP)
receptor on platelet cell membranes.
• The specific subtype of ADP receptor that clopidogrel irreversibly inhibits is P2Y12 and is
important in platelet aggregation and the cross-linking of platelets by fibrin.
• The blockade of this receptor inhibits platelet aggregation by blocking activation of the
glycoprotein IIb/IIIa pathway.
• The IIb/IIIa complex functions as a receptor mainly for fibrinogen and vitronectin but also
for fibronectin and von Willebrand factor. Activation of this receptor complex is the "final
common pathway" for platelet aggregation, and is important in the cross-linking of
platelets by fibrin.
186.
When does theaction of clopidogril start?
• Platelet inhibition can be demonstrated two hours after a single dose
of oral clopidogrel, but the onset of action is slow, so that a loading-
dose of 300-600 mg is usually administered.
187.
What is Cholesterolembolism (following
angiography)?
• Cholesterol embolisation is a well-documented complication of
coronary angiography
• Cholesterol emboli may break off causing renal disease
• Seen more commonly in arteriopaths, abdominal aortic aneurysms
188.
What are thefeatures of cholesterol
embolism following angiography?
• Eosinophilia
• Purpura
• Renal failure
• Livedo reticularis (is a common cutaneous finding consisting of a mottled
reticulated vascular pattern that appears like a lace-like purplish discoloration of
the lower extremities, caused by swelling of (venules) in the skin, which makes
them more visible)
189.
What is Livedoreticularis?
• Livedo reticularis (is a common cutaneous finding consisting of a mottled
reticulated vascular pattern that appears like a lace-like purplish discoloration of
the lower extremities, caused by swelling of (venules) in the skin, which makes
them more visible)
190.
What is Supraventriculartachycardia (SVT)?
• Supraventricular tachycardia (SVT): Whilst strictly speaking the term
supraventricular tachycardia (SVT) refers to any tachycardia that is not ventricular
in origin the term is generally used in the context of paroxysmal SVT.
• Episodes are characterized by the sudden onset of a narrow complex tachycardia,
typically an atrioventricular nodal re-entry tachycardia (AVNRT).
• Other causes include Atrioventricular reciprocating tachycardia (AVRT) and
junctional tachycardias.
• AVRT includes Wolff-Parkinson-White (WPW) syndrome
191.
What is theacute management of
supraventricular tachycardia?
• Vagal maneuvers: e.g. Valsalva maneuver
• Adenosine 6mg then 12mg then 12mg - contraindicated in asthmatics -
verapamil is a preferable option (if no control) then
• Electrical cardioversion
192.
What is thedrugs used for secondary
prevention of supraventricular
tachycardia?
• Beta-blockers (Sotalal)
• Flecainide.
• Radio-frequency ablation
193.
How to differentiatebetween causes of
supraventricular Tachycardia (AVRT Vs AF) using
Adenosine?
• Atrioventricular re-entrant (AVRT) and atrioventricular nodal re-entrant
tachycardia (AVNRT) may terminate with adenosine.
• Transient atrioventricular (AV) block will unmask atrial fibrillation, atrial flutter
and atrial tachycardia but is unlikely to terminate them.
194.
What is prematureventricular contraction?
• It is a relatively common event where the heartbeat is initiated by Purkinje fibres
in the ventricles rather than by the sinoatrial node, the normal heartbeat
initiator.
• The electrical events of the heart detected by the electrocardiogram allow a PVC
to be easily distinguished from a normal heart beat.
• A PVC may be perceived as a "skipped beat" or felt as palpitations in the chest
195.
Premature ventricular contractionis usually
insignificant unless?
• Occurring frequently ( 6 beats/min )
• Short runs of ventricular tachycardia (V. Tach)
• Bigeminal rhythm
• Associated with serious organic heart disease
• Left ventricular decompensation (Decompensated Heart Failure)
• R-on-T phenomenon
196.
What is AtrialFibrillation?
• Atrial fibrillation (AF or A-fib) is the most common cardiac
arrhythmia (irregular heart beat).
• It may cause no symptoms, but it is often associated
with palpitations, fainting, chest pain, or congestive heart failure.
• However, in some people atrial fibrillation is caused by
otherwise idiopathic or benign conditions.
197.
Which is betterin Atrial Fibrillation, Rate
control or Rhythm control?
• when managing atrial fibrillation (AF), rhythm control strategy alone
has no survival benefit over a rate control strategy as long as high-risk
patients are anticoagulated
• rate control is not inferior to rhythm control for prevention of death
and cardiovascular morbidity in patients with persistent AF after
electrical cardioversion.
WHAT ARE THEQUESTIONS in AF?
• 1- will you rate control (more than 65 and IHD) or will cardiovert?
• A- decided to Rate (Beta Calcium digoxin)…. Then use the CHAD2
score to know if u r giving warfarin or only asprin
• B- decided to Cardiovert (then u should ask is it more than 48 hours
or less…. Then proceed as the slides
200.
What are theAgents with proven efficacy in the
pharmacological cardioversion of atrial
fibrillation?
• Amiodarone
• Flecainide (if no structural heart disease)
• Others (less commonly used in UK): quinidine, dofetilide, ibutilide,
propafenone
201.
What is theeffect of Flecanide on Atrial
Fibrillation?
• Flecanide is a pure sodium channel blocker which prolongs the cardiac action potential
to slow conduction. It is recognised to increase the risk of AF transforming into
flutter.
• Flutter with 1:1 conduction would result in a ventricular rate of 300 /min which is
impossible to conduct via the AV node. However, because flecanide slows the rate of
cardiac conduction it means that if a patient develops atrial flutter the atrial rate will
not be 300 /min, but more likely around 200 /min which then could conduct via the AV
node at a 1:1 ratio.
• For this reason patients should always be co-prescribed a beta blocker to reduce risk
if this happens, and you wonder if this was the tablet that had recently been stopped.
202.
What are theAgents with less proven efficacy
in the pharmacological cardioversion of atrial
fibrillation?
• Beta-blockers (including sotalol)
• Calcium channel blockers
• Digoxin
• Disopyramide
• Procainamide
203.
What is thetreatment of Atrial fibrillation if
occurs since less than 48 hours?
• If atrial fibrillation (AF) is of less than 48 hours onset patients should be
heparinised and a transthoracic echocardiogram performed to exclude a
thrombus.
• Following this, patient may be cardioverted, either:
• Electrical - 'DC cardioversion'
• Pharmacology - amiodarone if structural heart disease, flecainide in those without structural
heart disease
• Following electrical cardioversion if AF is confirmed as being less than 48 hours
duration then further anticoagulation is unnecessary
204.
What is thetreatment of Atrial fibrillation if
occurs since more than 48 hours?
• If AF is of greater than 48 hours then patients should have therapeutic anticoagulation for at
least 3 weeks.
• If there is a high risk of cardioversion failure (e.g. previous failure or AF recurrence) then it is
recommended to have at least 4 weeks amiodarone or sotalol prior to electrical cardioversion.
• If there was very acute history on presentation and the patient was in significant heart failure
then DC cardioversion would be appropriate, as per Advanced Life Support guidelines.
• Following electrical cardioversion patients should be anticoagulated for at least 4 weeks. After
this time decisions about anticoagulation should be taken on an individual basis depending on
the risk of recurrence.
205.
What are theAgents used to control rate in
patients with atrial fibrillation?
• Beta-blockers (sotalol)
• Calcium channel blockers
• Digoxin
206.
What are theAgents used to maintain sinus
rhythm in patients with a history of atrial
fibrillation?
• Sotalol
• Amiodarone
• Flecainide
• Others (less commonly used in UK): disopyramide, dofetilide, procainamide,
propafenone, quinidine
207.
What are theFactors favoring rate control in
management of patient with Atrial
fibrillation?
• Older than 65 years
• History of ischemic heart disease
208.
What are theFactors favoring (cardioversion) in
management of patient with Atrial fibrillation?
• Younger than 65 years
• Symptomatic
• First presentation
• Lone AF or 2ndry AF (e.g. alcohol)
• Congestive heart failure
209.
What can yougive to a patient with Atrial
Fibrillation who is refuing to take warfarin?
• Watchmans device: A possible procedure can be offered to close off the left
atrial appendage (LAA), where the majority of thrombi form in patients with
atrial fibrillation.
• A catheter-based procedure delivers the device to the LAA via the septum but
requires 30 to 45 days of anticoagulation while the device is endothelialised.
210.
What is theclassification of Atrial fibrillation?
• It is recommended that AF be classified into 3 patterns:
• First detected episode (irrespective of whether it is symptomatic or self-terminating)
• Recurrent episodes, when a patient has 2 or more episodes of AF. If episodes of AF terminate
spontaneously then the term paroxysmal AF is used (the most AF that benefit from Beta
blocker). Such episodes last less than 7 days (typically < 24 hours). If the arrhythmia is not self
terminating then the term persistent AF is used. Such episodes usually last greater than 7 days
• In permanent AF there is continuous atrial fibrillation which cannot be cardioverted or if attempts
to do so are deemed inappropriate. Treatment goals are therefore rate control and
anticoagulation if appropriate
211.
What is themanagement of paroxysmal atrial
fibrillation?
• Bisoprolol is recommended as initial prophylaxis against further episodes of
paroxysmal atrial fibrillation by both NICE and the European Society of
Cardiology.
• Many patients do not however want to commit to long term therapy, and for this
reason, electrophysiological studies, coupled with possible ablation is an
increasingly popular option.
212.
What is HolidayHeart Syndrome?
• Supraventricular arrhythmias (including AF) secondary to acute
alcohol intake are well characterized and have been termed 'holiday
heart syndrome'.
• No specific treatment is required
213.
What is TheCHAD2 score?
• It’s a score used to tune the management of Atrial fibrillation
214.
Explain The CHAD2score (to decide if you are
going to give anticoagulants for AF controlled by Rate
not the cardioversion)?
• Condition Points
• C Congestive heart failure 1
• H Hypertension (or treated hypertension) 1
• A Age > 75 years 1
• D Diabetes 1
• S2 Prior Stroke or TIA 2
215.
What is theAnticoagulation therapy in Atrial
fibrillation according to score?
• 0: Aspirin
• 1: Aspirin or warfarin, depending on patient preference and individual factors
• 2: Warfarin if not contraindicated
• The guidelines have changed, for secondary prevention for stroke (after a TIA or stroke
happened) Aspirin is no longer used in stages 0 or 1, In patients with atrial fibrillation,
anticoagulation should be with either warfarin, or one of the newer anticoagulant drugs licensed
in the UK; dabigatran (Pradaxa), rivaroxaban (Xarelto) or apixaban (Eliquis). (You choose between
the agents according to the state of the patient)
216.
What is Dabigatran?
•Dabigatran is a direct thrombin inhibitor and holds a UK licence for the
prophylaxis of stroke in AF patients who have either had a previous stroke or
transient ischaemic attack (TIA), symptomatic heart failure, hypertension,
diabetes or in those aged over 75 years.
• It requires no therapeutic monitoring of coagulation tests and needs no loading
regime when used in thromboprophylaxis.
• It does have an unfavourable bleeding profile and has no validated reversal
agent in the event of catastrophic haemorrhage so is becoming less favoured.
217.
What are Rivaroxabanand apixaban ?
• Rivaroxaban and apixaban are both direct inhibitors of activated factor X (Xa), the
preceding factor which activates thrombin in the clotting cascade.
• Both have UK licenses for the thromboprophylaxis of stroke in AF patients with
similar indications as for dabigatran, although rivaroxaban can be used
preferentially by the patient if it is felt that they have failed to maintain a stable INR
with warfarin or if they prefer this drug over warfarin.
• Both apixaban and rivaroxaban lack a reversal agent in the occurrence of major
bleeding but studies have shown a reduced incidence of bleeding compared to both
warfarin and dabigatran. Neither drug requires monitoring nor loading when used
for this indication, making them popular choices with patients.
218.
Can we useDabigatran, Rivaroxaban or apixaban
for stroke prophylaxis in patients with AF and a
structural valve disease?
• No, all three agents do not have UK licences for AF in patients with
structural heart disease.
• Warfarin is the only licensed anticoagulant drug for stroke prevention
in AF in those with structurally abnormal valves
219.
What are theNICE2006 guidelines on
anticoagulation therapy in case of Atrial
Fibrillation (Older Guidelines)?
• Following a stroke or transient-ischemic attack (TIA) warfarin should be given as
the anticoagulant of choice.
• Aspirin/dipyridamole should only be given if needed for the treatment of other
comorbidities
• In acute stroke patients, in the absence of hemorrhage, anticoagulation therapy
should be commenced after 2 weeks.
• If imaging shows a very large cerebral infarction then the initiation of
anticoagulation should be delayed
220.
What is VentricularTachycardia?
• Ventricular tachycardia (V-tach or VT) is a tachycardia, or fast heart
rhythm, that originates in one of the ventricles of the heart.
• The ventricles are the main pumping chambers of the heart. This is a
potentially life-threatening arrhythmia because it may lead
to ventricular fibrillation, asystole, andsudden death.
221.
What are thetypes of ventricular
Tachycardia?
• The are two main types of VT:
• Monomorphic VT: most commonly caused by myocardial infarction
• Polymorphic VT: A subtype of polymorphic VT is torsades de pointes which is
precipitated by prolongation of the QT interval. The causes of a long QT interval
are listed
222.
What should youdo to a patient with V-Tach?
• If the patient has adverse signs (systolic BP <90 mmHg, chest pain,
heart failure or rate > 150 beats/min) then immediate cardioversion is
indicated.
• In the absence of such signs antiarrhythmics may be used. If these
fail, then electrical cardioversion may be needed with synchronised
DC shocks
223.
What are theFeatures suggesting Ventricular
Tachycardia rather than Supra Ventricular
Tachycardia with aberrant conduction?
• AV dissociation
• Fusion or capture beats
• Positive QRS concordance in chest leads
• Marked left axis deviation
• History of IHD
• Lack of response to adenosine or carotid sinus massage, QRS > 160 ms
What is thedrug therapy of ventricular
tachycardia?
• First line is Amiodarone (bolus then infusion): ideally administered
through a central line
• Second line if Amiodarone failed: Lidocaine (bolus then infusion): use
with caution in severe left ventricular impairment
• Procainamide
• If Hemodynamically unstable you should give DC shock
226.
Should you giveVerapamil to treat
Ventricular Tachycardia?
• VERAPAMIL SHOULD NOT BE USED IN VT
• Verapamil should never be given to a patient with a broad complex tachycardia as
it may precipitate ventricular fibrillation in patients with ventricular tachycardia.
• Adenosine is sometimes given in this situation as a 'trial' if there is a strong
suspicion the underlying rhythm is supraventricular tachycardia with aberrant
conduction
227.
What is thetreatment of V-Tach with digitalis
toxicity?
• Treat with lidocaine and phenytoin
• Avoid Amiodarone and Procainamide (increase digitalis toxicity)
• D/C shock when all measures fail (but usually unsuccessful)
228.
What is thenext step if drug therapy for V-
tach failed?
• Electrophysiological study (EPS)
• Implantable cardioverter-defibrillator (ICD) this is particulary indicated in patients
with significantly impaired LV function
229.
What is TorsadesDe Pointes ?
• Torsades De Pointes ('twisting of the points') is a rare arrhythmia
associated with a long QT interval.
• It may deteriorate into ventricular fibrillation and hence lead to
sudden death
230.
What are therisk factors for developing
Torsades De Pointes ?
• Females
• Decreased HR
• CHF
• Digoxin
• Hypokalaemia, hypomagnesaemia
• Prolonged QT and Subclinical long QT syndrome
• Severe alkalosis
• Recent conversion from AF
231.
What are theCauses of long QT interval?
• Congenital: Jervell-Lange-Nielsen syndrome, Romano-Ward syndrome
• Antiarrhythmics: amiodarone, sotalol, class I-a antiarrhythmic drugs
• Tricyclic antidepressants
• Antipsychotics
232.
What are theDrug Causes of long QT
interval?
• Chloroquine
• Terfenadine
• Erythromycin
• Electrolyte: Hypocalcemia, Hypokalemia, Hypomagnesemia
• Myocarditis
• Hypothermia
• Subarachnoid hemorrhage
233.
What is thetreatment of Torsades De
Pointes?
• IV magnesium sulphate (It replaces the Magnesium)
• Correct K+ if hypo
• Override pacing (set pacemaker to be faster than patient rate then decrease the
rate)
• D/C shock
234.
What is themechanism by which Magnesium
helps with Torsades?
• Pharmacotherapy for polymorphic ventricular tachycardia is magnesium, which
decreases calcium influx, reducing the amplitude of the VT and helping
terminate runs of torsades.
• It is effective even when serum magnesium is normal.
235.
What is MultifocalAtrial Tachycardia (MAT)?
• Multifocal Atrial Tachycardia (MAT) may be defined as irregular cardiac rhythm
caused by at least three different sites in the atria, which may be demonstrated
by morphologically distinctive P waves.
• It is more common in elderly patients with chronic lung disease (e.g COPD)
236.
What is thetreatment of Multifocal Atrial
Tachycardia (MAT)?
• Correction of hypoxia and electrolyte disturbances
• Rate-limiting calcium channel blockers are often used first-line
• Cardioversion and digoxin are not useful in the management of MAT
237.
How to manageperi-arrest tachycardias?
• Following basic ABC assessment, patients are classified as being stable or
unstable according to the presence of any adverse signs:
• Systolic BP < 90 mmHg
• Decreased conscious level
• Chest pain
• Heart failure
• If any of the above adverse signs are present then synchronised DC shocks should
be given
• Treatment following this is given according to whether the QRS complex is
narrow or broad and whether the rhythm is regular or irregular.
238.
How to manageperi-arrest tachycardias
(Broad-complex- Regular)?
• Assume ventricular tachycardia (unless previously confirmed SVT
with bundle branch block)
• Loading dose of amiodarone followed by 24 hour infusion
239.
How to manageperi-arrest tachycardias
(Broad-complex- Irregular)?
• AF with bundle branch block - treat as for narrow complex
tachycardia
• Polymorphic VT (e.g. torsade de pointes) - IV magnesium
240.
How to manageperi-arrest tachycardias
(Narrow-complex- Irregular)?
• Probable atrial fibrillation
• If onset < 48 hr: consider electrical or chemical cardioversion
• >48 HR: Rate control (e.g. Beta-blocker or digoxin) and
anticoagulation
241.
How to manageperi-arrest tachycardias
(Narrow-complex- Regular)?
• Vagal manoeuvres followed by IV adenosine
• If above unsuccessful consider diagnosis of atrial flutter and control
rate (e.g. Beta - blockers)
242.
What are theguidelines for treating
Bradycardia and Peri-Arrest?
• Bradycardia and Peri-Arrest:
• Identifying the presence of signs indicating hemodynamic compromise - 'adverse
signs'
• Identifying the potential risk of asystole
243.
What are thefactors that indicate
Hemodynamic compromise in Bradycardia?
• The following factors indicate hemodynamic compromise and hence the need for
treatment:
• Heart rate < 40 bpm
• Systolic blood pressure < 100 mmHg
• Heart failure
• Ventricular arrhythmias requiring suppression
244.
What should youdo in case of identified
Hemodynamic compromise in Bradycardia?
• Atropine is the first line treatment in this situation.
• If this fails to work, or there is the potential risk of asystole then transvenous
pacing is indicated
245.
What should youdo in case of identified
Hemodynamic compromise in Bradycardia in a
patient with previous Heart transplantation?
• Atropine is usually the first line treatment for bradycardia and if that fails then
consider transcutaneous or transvenous pacing.
• However, in patients with heart transplant atropine is
contraindicated.
• The hearts of these patients are denervated and do not respond to vagal
blockade by atropine, which might precipitate paradoxical sinus arrest of high-
grade block. In these cases, theophyline intravenousely is indicated.
246.
What is therisk of Asystole in case of
complete heart block with narrow complex
QRS?
• Complete heart block with a narrow complex QRS complex carries
the least risk of asystole as the atrioventricular junctional
pacemaker may provide a hemodynamically acceptable and stable
heart rate
247.
Which conditions carrythe risk of Asystole as
a result of Bradycardia?
• Complete heart block
• Recent asystole
• Mobitz type II heart block
• Symptomatic 2nd degree
• Ventricular pause > 3 seconds
248.
If a patientrecords episodes of complete heart
block and pauses for more than 3 seconds on 24
hrs ECG, how should he be managed?
• pauses lasting for greater than 3 seconds associated with episodes of complete
heart block are indicators for permenant pacemaker
249.
What should youdo for a patient with Bradycardia that
may develop into Asystole if there is a delay to make a
transvenous pacing available?
• Atropine, up to maximum of 3mg
• Transcutaneous pacing
• Adrenaline infusion titrated to response
250.
What is thedifference between Mobitz type I
and Mobitz type II?
• There are two types of second degree heart block:
• Mobitz type I (Wenckebach phenomenon), which is characterised by progressive
prolongation of the PR interval until a P wave fails to conduct to the ventricle,
and
• Mobitz type II, which is characterised by an intermittent failure of the P wave to
stimulate a QRS complex at regular intervals — the PR interval is constant.
• Atropine may be used in selected cases of transient AV block (bradycardia with
symptoms as per the acute life support guidelines*), but in general permanent
cardiac pacing has replaced medical interventions where the patient is
symptomatic with their AV block.
251.
A patient withInferior MI develops Mobitz
and a patient with anterior MI develops it,
what is the difference?
• Atrioventricular (AV) block is commonly associated with inferior myocardial
infarctions as the blood supply to the AV node arises from the right coronary
artery, which is the culprit vessel in most cases of inferior MIs. It is thought to be
of no prognostic significance in this case and usually resolves in the first 24 h
• In contrast AV blocks in the context of anterior MIs convey a poor prognosis as
they signify an extensive event.
252.
What are thefeatures of complete Heart
Block?
• Syncope
• Heart failure
• Regular bradycardia (30-50 bpm)
• Wide pulse pressure
• JVP: cannon waves in neck
• Variable intensity of S1.
253.
What is Bifasicularand Trifasicular Block?
• Bifascicular and trifascicular block refer to conduction disturbances below the
atrioventricular (AV) node in which two or more of the fascicles of the left bundle
branch and the right bundle branch are involved.
• It has been suggested that unexplained syncope in the presence of bifascicular or
trifascicular block is an indication for a permanent pacemaker.
254.
What is TrifasicularBlock?
• Trifasicular Block: The PR interval is grossly prolonged (1st degree block) and
there is an RSR complex in V1 (RBBB) and a left anterior hemi-block (LAHB is
diagnosed when QRS in lead II is negative).
• The combination of RBBB, LAHB and long PR interval has been called trifasicular
block.
255.
What are theIndications for a Temporary
Pacemaker?
• Symptomatic/hemodynamically unstable bradycardia, not responding to atropine
• Post-ANTERIOR MI: type 2 or complete heart block
• Trifascicular block prior to surgery
256.
post-Inferior MI completeheart block is an
Indications for a Temporary Pacemaker, T/F?
• False
• post-Inferior MI complete heart block is common and can be managed
conservatively if asymptomatic and hemodynamically stable
257.
What are theIndications of Implantable
Cardiac Defibrillators (IDC)?
• Long QT syndrome
• Hypertrophic obstructive cardiomyopathy (HOCM)
• Previous cardiac arrest due to VT/VF
• Previous myocardial infarction with non-sustained VT on 24 hr monitoring,
inducible VT on electrophysiology testing and ejection fraction < 35%
• Brugada syndrome
258.
What is LongQT Syndrome (LQTS)?
• Long QT Syndrome (LQTS) is an inherited condition associated with delayed
repolarization of the ventricles.
• It is important to recognise as it may lead to ventricular tachycardia and can
therefore cause collapse/sudden death.
• The most common variants of LQTS (LQT1 & LQT2) are caused by defects in
subunit of the slow delayed rectifier potassium channel.
• A normal corrected QT is less than 440 ms in males and 450 ms in females
259.
What are thecauses of inherited Long QT
syndrome?
• Six mutations (LQT1–6) have been identified in association with the
Romano–Ward syndrome.
• LQT1 and LQT2 mutations make up around 87% of cases of Romano–
Ward syndrome and are associated with cardiac potassium-channel
gene mutations.
• JLN mutations (Jervell–Lange-Nielsen syndrome) tend to be
associated with deafness.
260.
What are thedifferent presentations for patients
with inherited Long QT according to the different
types of mutations they have?
• Patients with LQT1 usually have cardiac events preceded by exercise or
swimming. Sudden exposure of the patient's face to cold water is thought to
elicit a vagotonic reflex.
• Patients with LQT2 may have arrhythmic events after an emotional event,
exercise, or exposure to auditory stimuli (eg, door bells, telephone ring).
• Patients with LQT3 usually have events during night sleep.
261.
Blockage of K+channels causes prolongation of
QT, T/F?
• True
262.
What are thedrug causes of Long QT
Syndrome (LQTS)?
• Amiodarone
• Sotalol
• Class I-a antiarrhythmic
• Tricyclic antidepressants
• Chloroquine
• Terfenadine
• Macrolide (erythromycin)
• Quinolones
263.
What are thecongenital causes of Long QT
Syndrome (LQTS)?
• Jervell-Lange-Nielsen syndrome (includes deafness and is due to an abnormal
potassium channel)
• Romano-Ward syndrome (no deafness)
264.
What are thecauses of Long QT Syndrome
(LQTS)?
• Electrolyte:
• Hypocalcemia, Hypokalemia, Hypomagnesemia
• Acute MI
• Myocarditis
• Hypothermia
• Subarachnoid hemorrhage
265.
What are thefeatures of Long QT Syndrome
(LQTS)?
• May be picked up on routine ECG or following family screening
• Long QT1 - usually associated with exertional syncope, often swimming
• Long QT2 - often associated with syncope occuring following emotional stress,
exercise or auditory stimuli
• Long QT3 - events often occur at night or at rest (associated with brady, so
pacemaker may be beneficial)
• Long QT4 – associated with Parox. AF
• Sudden cardiac death
266.
What is thetreatment of Long QT Syndrome
(LQTS)?
• Avoid drugs which prolong QT and other precipitants if appropriate (e.g.
Strenuous exercise)
• 1st line pharmacological therapy is Mg+ IV (bolus then infusion)
• Beta-blockers (avoid sotalol as it causes prolonged QT)
• Implantable cardioverter defibrillators in high risk cases (if Beta-blockers fail)
• Left stellate sympathectomy (if -blockers fail or when there is multiple ICD
shocks)
267.
What is therole of Beta blockers in the
treatment of Long QT Syndrome (LQTS)?
• Beta-blockers decrease sympathetic activation from the left stellate ganglion.
• Beta-blockers also decrease the maximal heart rate achieved during exertion and
thereby prevent exercise-related arrhythmic events that occur in long QT
syndrome.
• Patients who experience ventricular arrhythmias or aborted sudden cardiac death despite beta-blocker
therapy should have an implantable cardioverter defibrillator (ICD) in addition to beta-blockers.
• Left stellate cardiac ganglionectomy is an invasive procedure and results in Horner’s syndrome. It is
performed in patients who have symptoms despite beta-blockers and have frequent shocks with ICD.
268.
What is therisk of prolonged QT in a case of
patient with common cold?
• A non-sedating antihistamine and classic cause of prolonged QT in a patient,
especially if also taking P450 enzyme inhibitor, e.g. Patient with a cold takes
terfenadine and erythromycin at the same time
269.
What is ArrhythmogenicRight Ventricular
Cardiomyopathy (ARVC)?
• Autosomal dominant
• It is a form of inherited cardiovascular disease which may present with syncope
or sudden cardiac death.
• It is generally regarded as the second most common cause of sudden cardiac
death in the young after hypertrophic cardiomyopathy.
270.
What is thepathophysiology of
Arrhythmogenic Right Ventricular
Cardiomyopathy (ARVC)?
• Inherited in an autosomal dominant pattern with variable expression
• The right ventricular myocardium is replaced by fibrofatty tissue
271.
What is thepresentation of Arrhythmogenic
Right Ventricular Cardiomyopathy (ARVC)?
• Palpitations
• Syncope
• Sudden cardiac death
272.
What are theinvestigations for Arrhythmogenic
Right Ventricular Cardiomyopathy (ARVC)?
• ECG abnormalities in V1-3, typically T wave inversion. An epsilon wave is found
in about 50% of those with ARV - this is best described as a terminal notch in the
QRS complex
• Echo changes are often subtle in the early stages but may show an enlarged,
hypokinetic right ventricle with a thin free wall
• Magnetic resonance imaging is useful to show fibrofatty tissue
273.
What is themanagement of Arrhythmogenic
Right Ventricular Cardiomyopathy (ARVC)?
• Drugs: sotalol is the most widely used antiarrhythmic
• Catheter ablation to prevent ventricular tachycardia
• Implantable cardioverter-defibrillator
274.
What is Naxosdisease?
• An autosomal recessive variant of ARVC (Arrhythmogenic Right
Ventricular Cardiomyopathy )
• A triad of ARVC, palmoplantar keratosis, and woolly hair
275.
What is Wolff-ParkinsonWhite (WPW)?
• Wolff-Parkinson White (WPW) syndrome is caused by a congenital accessory
conducting pathway between the atria and ventricles leading to atrioventricular
re-entry tachycardia (AVRT).
• As the accessory pathway does not slow conduction AF can degenerate rapidly to
VF
276.
How do patientswith Wolff-Parkinson White
(WPW) usually present?
• The majority of patients present with reciprocating tachycardias at 150–250
beats per minute, 15% present with atrial fibrillation and around 5% with atrial
flutter.
277.
What are theECG features of Wolff-Parkinson
White (WPW)?
• Short PR interval
• Wide QRS complexes with a slurred upstroke - 'delta wave'
• Left axis deviation if right-sided accessory pathway
• Right axis deviation if left-sided accessory pathway
278.
Why left axisdeviation occur with right sided
Wolff-Parkinson White (WPW) and vice
versa?
• Because of this picture, the side that the pathway will be in, will have a shorter
vector because of the opposing direction of the sided pathway, then the added
direction of the circling wave through the pathway will add to the vector on the
other side
279.
How to differentiatebetween type A and type B
Wolff-Parkinson White (WPW)?
• Type A (left-sided pathway): dominant R wave in V1, seen in the above ECG.
• Type B (right-sided pathway): no dominant R wave in V1
280.
What are thediseases that may be associated
with Wolff-Parkinson White (WPW)?
• HOCM
• Mitral valve prolapse
• Ebstein's anomaly
• Thyrotoxicosis
• Secundum ASD
281.
What is thetreatment of Wolff-Parkinson
White (WPW)?
• Definitive treatment: radiofrequency ablation of the accessory pathway
• Medical therapy: sotalol ????, disopyramide, amiodarone, flecainide
• For cardioversion: Flecainide is superior to Amiodarone
• DC cardioversion should be used early if the tachycardia is causing
haemodynamic comprise
282.
Which drugs shouldyou avoid in Wolff-
Parkinson White (WPW)?
• A simple mnemonic to remember for drugs to avoid in WPW syndrome is ABCD
(Adenosine, Beta -Blockers, Calcium Channel Blockers, Digoxin).
283.
in the majorityof cases, or in a question without
Specification, Wolff-Parkinson-White syndrome is
associated with left axis deviation, T/F?
• True
284.
When should youavoid giving sotalol as a
treatment for Wolff-Parkinson White (WPW)?
• sotalol should be avoided if there is coexistent atrial fibrillation as
prolonging the refractory period at the AV node may increase the rate
of transmission through the accessory pathway, increasing the
ventricular rate and potentially deteriorating into ventricular
fibrillation.
285.
Why should youavoid giving Adenosine,
verapamil, Digoxin with Wolff-Parkinson
White (WPW)?
• Adenosine should be avoided as blocking the AV node can
paradoxically increase ventricular rate resulting in fall in cardiac
output.
• “They may accelerate conduction down the accessory
pathway”
286.
Why should youavoid giving Verapamil and
digoxin with Wolff-Parkinson White (WPW)?
• Verapamil and digoxin should also be avoided in patients with Wolff-
Parkinson White as they may precipitate VT or VF.
287.
What is Catecholaminergicpolymorphic
ventricular tachycardia (CPVT)?
• Catecholaminergic polymorphic ventricular tachycardia (CPVT) is a form of
inherited cardiac disease associated with sudden cardiac death.
• It is inherited in an autosomal dominant fashion and has a prevalence of around
1:10,000.
288.
What is thepathophysiology of Catecholaminergic
polymorphic ventricular tachycardia (CPVT)?
• The most common cause is a defect in the ryanodine receptor (RYR2) which is
found in the myocardial sarcoplasmic reticulum
289.
What are thefeatures of Catecholaminergic
polymorphic ventricular tachycardia (CPVT)?
• Exercise or emotion induced polymorphic ventricular tachycardia resulting in
syncope
• Sudden cardiac death
• Symptoms generally develop before the age of 20 years
290.
What is themanagement of Catecholaminergic
polymorphic ventricular tachycardia (CPVT)?
• Beta-blockers
• Implantable cardioverter-defibrillator
291.
What is Brugadasyndrome?
• Brugada syndrome is a form of inherited cardiovascular disease with may present with
sudden cardiac death.
• BrS manifests with syncope and cardiac arrest typically occurring in the third and
fourth decade of life, and usually at rest or during sleep.
• It is inherited in an autosomal dominant fashion and has an estimated prevalence of
1:5,000-10,000.
• Brugada syndrome is more common in Asians.
292.
What is thepathophysiology of Brugada
syndrome?
• There are usually no structural abnormalities (Echo will be Normal) in
Brugada syndrome (BrS) patients and the disease may be defined as a pure
electrical abnormality of myocardial cells.
• A large number of variants exist
• Around 20-40% of cases are caused by a mutation in the SCN5a gene which
encodes the myocardial sodium ion channel protein
293.
What are theECG changes in Brugada
syndrome?
• Convex ST elevation V1-V3
• Partial right bundle branch block
• Changes may be more apparent following flecainide (providing additional sodium
channel blockade to that already pathologically present)
• Ajmaline (class Ia antiarrhythmic) is used to unmask hidden Brugada
294.
What is themanagement of Brugada
syndrome?
• Implantable cardioverter-defibrillator
• Quinidine is useful in VF storm (indicated by fast repeated ICD shocks)
295.
What is HypertrophicObstructive
Cardiomyopathy (HOCM)?
• It is an autosomal dominant disorder of muscle tissue caused by defects in the
genes encoding contractile proteins.
• The estimated prevalence is 1 in 500.
• Mutations to various proteins including Beta-myosin, Alpha-tropomyosin and
troponin T have been identified.
• Septal hypertrophy causes left ventricular outflow obstruction.
• It is an important cause of sudden death in apparently healthy individuals.
296.
What are thesymptoms of Hypertrophic
Obstructive Cardiomyopathy (HOCM)?
• Often asymptomatic
• Dyspnea, angina, syncope
• Sudden death (most commonly due to ventricular arrhythmias), arrhythmias,
heart failure
• Jerky pulse, large 'a' waves, double apex beat
• Ejection systolic murmur: increases with valsalva manoeuvre and decreases on
squatting
297.
What are thediseases associated with
Hypertrophic Obstructive Cardiomyopathy
(HOCM)?
• Friedreich's ataxia
• Wolff-Parkinson White
298.
What is theECG picture of Hypertrophic
Obstructive Cardiomyopathy (HOCM)?
• Left ventricular hypertrophy (LVH), Atrial enlargement (abnormal P morphology)
• Progressive T wave inversion, ST-T abnormalities, Deep Q waves
• Axis deviation (right or left)
• Prolonged PR or sinus bradycardia
• BBB (bundle brach block)
• Ectopic atrial rhythm
• Atrial fibrillation may occasionally be seen
299.
What are theEcho Features of Hypertrophic
Obstructive Cardiomyopathy (HOCM)?
• (Mr. Sam Ash):
• Mitral regurgitation (MR)
• Systolic anterior motion (SAM) of the anterior mitral valve leaflet
• Asymmetric hypertrophy (ASH)
300.
What are thebad prognostic factors associated
with Hypertrophic Obstructive Cardiomyopathy
(HOCM)?
• Syncope
• Family history of sudden death
• Young age at presentation
• Non-sustained ventricular tachycardia on 24 or 48-hour holter monitoring
• Abnormal blood pressure changes on exercise
• Increased Septal wall thickness, > 3cm
301.
What is themanagement of Hypertrophic
Obstructive Cardiomyopathy (HOCM)?
• Amiodarone
• Beta-blockers or verapamil for symptoms
• Cardioverter defibrillator
• Dual chamber pacemaker
• Endocarditis prophylaxis
302.
What is themanagement of symptoms of
cardiac failure in Hypertrophic Obstructive
Cardiomyopathy (HOCM)?
• Symptoms of cardiac failure respond to medical therapy with b-blockade; but
where the outflow gradient is greater than 50 mmHg, surgical myomectomy is
usually recommended, particularly if symptoms persist post beta blockade.
• Unfortunately surgery does not reduce the risk of arrhythmia.
• Patients prone to ventricular arrhythmias may be considered for implantable
defibrillator.
303.
What are thedrugs to avoid in Hypertrophic
Obstructive Cardiomyopathy (HOCM)?
• Nitrates
• ACE-inhibitors
• Inotropes
• Digoxin is contraindicated if there is significant LVOT gradient
304.
Hypertrophic obstructive cardiomyopathy(HOCM) is a more
common cause of sudden cardiac death than arrhythmogenic
right ventricular dysplasia (ARVD) 2nd most common, T/F?
• True
305.
What is DilatedCardiomyopathy (DCM)?
• Prevelance is 1% in adult – it to 10% at age of 80 yrs
• Annual mortality of cardiomyopathies and HF is 20%
• Dilated heart leading to systolic (+/- diastolic) dysfunction
• All 4 chambers affected but LV more than RV
• Features include arrhythmias, emboli, mitral regurgitation
• Absence of congenital, valvular or ischemic heart disease
306.
What are thecauses of Dilated
Cardiomyopathy (DCM)?
• Alcohol (significant improvement happens after stopping alcohol), Peripartum,
Hypertension, Inherited
• Infections e.g. Coxsackie A and B, HIV, diphtheria, parasitic
• Endocrine e.g. Hyperthyroidism
• Infiltrative* e.g. Hemochromatosis, sarcoidosis
• Neuromuscular e.g. Duchenne muscular dystrophy
• Nutritional e.g. Kwashiorkor, pellagra, thiamine/selenium deficiency
• Drugs e.g. Doxorubicin
307.
What do youknow about Inherited dilated
cardiomyopathy?
• Around a third of patients with DCM are thought to have a genetic predisposition
• A large number of heterogeneous defects have been identified
• The majority of defects are inherited in an autosomal dominant fashion although
other patterns of inheritance are seen
308.
Dilated Cardiomyopathy thatresulted from Alcohol
intake may improve with thiamine (best prognosis after
removing the cause), T/F?
• True
What are thefeatures of Restrictive
Cardiomyopathy?
• Similar to constrictive pericarditis
311.
What causes RestrictiveCardiomyopathy?
• Amyloidosis (e.g. Secondary to myeloma) - most common cause in
UK
• Hemochromatosis
• Loffler's syndrome
• Sarcoidosis
• Scleroderma
312.
Compare between Restrictive
cardiomyopathyvs Constrictive pericarditis
• In restrictive:
• Prominent apical pulse
• Absence of pericardial calcification on CXR
• Heart may be enlarged
• ECG abnormalities e.g. Bundle branch block, Q waves
313.
What is Peripartumcardiomyopathy?
• Peripartum cardiomyopathy causes left ventricular dysfunction and heart failure
during the last month of pregnancy (antepartum) or within the first 5 months’
postpartum.
• It is commonest in Africa where there is a prevalence of up to 1%. The cause is
unknown.
• Biopsy is not helpful.
314.
What is theprognosis of Peripartum
cardiomyopathy?
• Prognosis is reasonable with recovery of ventricular function in 50% of patients.
• Mortality rates range from 7-56% and are directly related to recovery of ejection
fraction.
• The risk of recurrence in further pregnancies is about 40%.
• If the ejection fraction does not recover and the patient remains symptomatic, a
heart transplant is usually considered.
315.
What is themanagement of Peripartum
cardiomyopathy?
• Management is supportive with digoxin, diuretics and vasodilators
• ACE inhibitors are not used during pregnancy as they can affect fetal renal
function.
• There is an increased incidence of thrombosis and it is common to anticoagulate
patients.
316.
What do youknow about Atrial Myxoma?
• 75% occur in left atrium
• More common in females
317.
What are thefeatures of Atrial Myxoma?
• Systemic: weight loss, fever, clubbing
• normocytic anaemia, a positional murmur and
• intracardiac calcification in the chest X-ray.
• Emboli
• Atrial fibrillation
• The history of fainting spells suggests transient left ventricular inflow
obstruction.
• Mid-diastolic murmur, 'tumour plop'
318.
What is themanagement of Atrial Myxoma?
• The patient should undergo urgent echocardiography if suspected and be
referred for surgery if the diagnosis of myxoma is confirmed, as complete
removal is curative.
319.
What are theFeatures of severe AS?
• Narrow pulse pressure, Slow rising pulse
• Delayed Ejection Systolic Murmer
• Soft/absent S2
• S4
• Thrill
• Increased Duration of murmur
• Left ventricular hypertrophy or failure
320.
Left ventricular systolicdysfunction will result in a
decreased flow-rate across the aortic valve and hence a
quieter murmur and low gradient on Echo, T/F?
• True
321.
What are thecauses of Aortic Stenosis?
• Degenerative calcification (most common cause in elderly patients)
• Bicuspid aortic valve (most common cause in younger patients)
• William's syndrome (supravalvular aortic stenosis)
• Post-rheumatic disease
• Subvalvular: HOCM
322.
Which test wouldyou use to assess the
severity of Aortic stenosis in severe Left
ventricular failure?
• Dobutamine echo is used to assess the severity of AS in severe LVSF impairment
• patient has severe left ventricular (LV) dysfunction, and calculated valve area in such patients can be
falsely low because low cardiac output reduces the valve opening forces. It is important to distinguish
patients with true severe aortic stenosis (AS) with secondary LV dysfunction from those who have a
falsely low calculated aortic valve area because of low cardiac output Patients with truly severe AS
manifest an increase in transaortic pressure gradient while the valve surface area remains the same
during dobutamine infusion; while those with falsely low calculated valve area manifest an increase in
calculated valve surface area.
• Patients with >20% increase in stroke volume after dobutamine means better
prognosis post surgery compared to those with no LV contractile reserve.
323.
What is themanagement of Aortic Stenosis?
• If asymptomatic then observe the patient is general rule
• If symptomatic then valve replacement
• If asymptomatic but valvular gradient > 50 mmHg and with features such as left
ventricular systolic dysfunction then consider surgery
• Balloon valvuloplasty is limited to patients with critical aortic stenosis who are
not fit for valve replacement
324.
What is themanagement of symptomatic
Aortic Stenosis in patients with significant
coronary artery insufficiency?
• Aortic valve replacement and a concomitant bypass grafting
325.
What is Heyde’ssyndrome?
• Heyde’s syndrome: a well-known association between microcytic anemia and
calcific AS.
• The treatment is to replace the valve, as the mechanism is thought to be due to
destruction of von Willebrand’s factor as the platelets traverse the stenosed
valve resulting in bleeding per rectum.
326.
What are thefeatures of Aortic Regurgitation
(AR)?
• Early diastolic murmur
• Collapsing pulse
• Wide pulse pressure
• Mid-diastolic Austin-Flint murmur in severe AR - due to partial closure
of the anterior mitral valve cusps caused by the regurgitation streams
327.
What are thecauses of Aortic Regurgitation
(AR) (due to valve disease)?
• Rheumatic fever
• Infective endocarditis
• Connective tissue diseases e.g. RA/SLE
• Bicuspid aortic valve
328.
What are thecauses of Aortic Regurgitation (AR)
(due to aortic root disease)?
• Aortic dissection
• Spondylarthropathies (e.g. Ankylosing spondylitis)
• Hypertension
• Syphilis
• Marfan's, Ehler-Danlos syndrome
329.
What is themanagement of Aortic
Regurgitation?
• Vasodilator therapy (angiotensin-converting enzyme inhibitors or nifedipine)
should be given to patients who do not have indications for Valve replacement.
• Valve replacement if:
• symptomatic
• Asymptomatic with Left ventricle Systolic Flow <50% +
• dilated LV (EDD > 75mm – ESD>55mm)
330.
When does Acutemitral regurgitation occur?
• Acute mitral regurgitation may occur post myocardial infarction (MI)
due to ruptured chordae tendonae.
• Patients present with hypotension, tachycardia and left ventricular
failure and with a systolic murmur loudest at the apex.
• “VSD occurring after MI present with systolic murmur is heard
loudest at the left sternal edge”
331.
What is themanagement of Acute mitral
regurgitation?
• If blood pressure allows, patients benefit from volume reduction using diuretics
and initiation of angiotensin converting enzyme (ACE) inhibitor therapy.
• Surgical repair in post-MI patients carries high operative risk.
332.
What is theepidemiology of Mitral Valve
prolapse?
• Mitral Valve Prolapse is common, occurring in around 5-10 % of the population.
• It is usually idiopathic but may be associated with a wide variety of
cardiovascular disease and other conditions
333.
What are thediseases that are associated
with Mitral Valve prolapse?
• Congenital heart disease: PDA, ASD
• Cardiomyopathy
• Turner's syndrome
• Marfan's syndrome, Fragile X
• Osteogenesis imperfecta
• Pseudoxanthoma elasticum
• Wolff-Parkinson White syndrome
• Long-QT syndrome
334.
What are thefeatures of Mitral Valve
prolapse?
• Patients may complain of atypical chest pain or palpitations
• Mid-systolic click (occurs later if patient squatting)
• Late systolic murmur crescendo-decrescendo murmur heard loudest at the lower
left sternal edge (longer if patient standing)
• Complications: mitral regurgitation, arrhythmias (including long QT), emboli,
sudden death
335.
What is themanagement of Mitral Valve
prolapse?
• Patients > 75 years who are in AF or with LVSF impairment, should be referred to
surgical assessment as early as possible
• TOE (transesophageal echo)can tell if the valve is for repair or replacement, can be
done intraoperatily
• Follow up is crucial as 15% of MVP patients develop the most serious complication
after 15 years period of being prolapsed (TIA, Ischemic Stokes)
• Mild to moderate MVP with normal LVSF give Beta blockers + echo
follow up every 2-3 years
336.
What causes MitralStenosis?
• It is said that the causes of mitral stenosis are rheumatic fever, rheumatic fever
and rheumatic fever.
• Rarer causes that may be seen in the MRCP include mucopolysaccharidoses,
carcinoid and endocardial fibroelastosis
337.
What are thefeatures of Mitral Stenosis?
• Mid-diastolic murmur (best heard in expiration) with the presence of a bifid P
wave (P-mitrale) on the electrocardiogram (ECG)
• Loud S1, opening snap
• Low volume pulse
• Malar flush
• Atrial fibrillation
338.
What are thefeatures of SEVERE mitral
stenosis?
• Increased Length of murmur
• Opening snap becomes closer to S2
339.
What are thefeatures of Mitral stenosis on
Echocardiography?
• The normal cross sectional area of the mitral valve is 4-6 cm2.
• A 'tight' mitral stenosis implies a cross sectional area of < 1 cm2.
340.
What are thecontraindications to
Percutaneous Balloon Valvotomy in treating
Mitral Stenosis?
• It is contraindicated in:
• Moderate to severe mitral regurgitation
• Left atrial thrombus
• Heavily calcified mitral valve
• Concomitant coronary artery or other valve disease requiring surgery.
341.
What is thetreatment of severe Mitral
Stenosis?
• Percutaneous Balloon Valvotomy is used to treat sever M.S.
342.
What is Lutembacher’ssyndrome?
• Lutembacher’s syndrome: is a syndrome characterized by both MS & ASD. Both
conditions may be congenital and occur concurrently, or the MS may occur as a result of
rheumatic fever or other cause.
• Incidence of Lutembacher’s syndrome is higher in women due to the higher incidence of
congenital ASD.
• Cardiac signs are mixed due to the two concurrent lesions.
• Presentation is typically in later life, with fatigue or atrial fibrillation.
• Ideally, surgery should be performed as early as possible due to the risks of Eisenmenger’s
syndrome if untreated.
343.
What are thefeatures of Lutembacher’s
syndrome?
• small volume pulse, distended jugular veins, left parasternal lift, a tapping apex
impulse, and there is a loud first heart sound and a mitral early- to mid-diastolic murmur.
• There also appears to be a mid-diastolic tricuspid murmur
344.
What are thesigns of Tricuspid
Regurgitation?
• Pan-systolic murmur
• Giant v waves in JVP
• Pulsatile hepatomegaly
• Left parasternal heave
345.
What are thecauses of Tricuspid
Regurgitation?
• Right ventricular dilation
• Pulmonary hypertension e.g. COPD
• Rheumatic heart disease
• Infective endocarditis (especially intravenous drug users)
• Ebstein's anomaly
• Carcinoid syndrome
346.
What are thecommonest valves to need
replacements?
• The most common valves which need replacing are the aortic and mitral valve.
• There are two main options for replacement: biological (bioprosthetic) or
mechanical.
347.
What do youknow about Biological
(bioprosthetic) valves?
• Usually bovine or porcine in origin
• Major disadvantage is structural deterioration and calcification over time. Most
older patients ( > 65 years for aortic valves and > 70 years for mitral valves)
receive a bioprosthetic valve
• Long-term anticoagulation not usually needed.
• Warfarin may be given for the first 3 months depending on patient factors. Low-
dose aspirin is given long-term.
348.
What do youknow about Mechanical valves?
• The most common type now implanted is the bileaflet valve. Ball-and-cage valves
are rarely used nowadays
• Mechanical valves have a low failure rate
• Major disadvantage is the increased risk of thrombosis meaning long-term
anticoagulation is needed. Aspirin is normally given in addition unless there is a
contraindication.
• Target INR
• Aortic: 2.0-3.0
• Mitral: 2.5-3.5
349.
Should you giveantibiotic prophylaxis for
patient with prosthetic valves that are to
have dental or common procedures?
• Following the 2008 NICE guidelines for prophylaxis of endocarditis antibiotics are
no longer recommended for common procedures such as dental work
350.
What is ProstheticValve Thrombosis (PVT)?
• Prosthetic Valve Thrombosis (PVT): This complication occurs in 0.03 to 5.5%
annually with equal frequency in bioprosthesis and mechanical valves.
• It is more common in mitral prosthesis and with subtherapeutic anticoagulation,
this resulting in shock.
351.
How to diagnoseProsthetic Valve Thrombosis
(PVT)?
• The best diagnostic modality is transoesophageal echocardiography
• Transthoracic echocardiography is the initial choice in sick patients, and if
adequate visualisation is not obtained TEE can be done.
352.
What is themanagement of Prosthetic Valve
Thrombosis (PVT)?
• Thrombolytic therapy should be given for patients in pulmonary edema or
hypotension (complication).
• In stable patients, surgery is a better option for left-sided PVT, while right-sided
PVT should be treated with thrombolytic agents.
• Serial echocardiography should be performed, and if the response is inadequate
repeat thrombolytic therapy can be given.
353.
Can you summarizein short note how to deal
with the different types of Aortic dissection?
• Type A - ascending aorta - control BP(IV labetalol) + surgery
• Type B - descending aorta - control BP(IV labetalol)
354.
What are thetypes of Aortic Disection?
• Type A- Ascending aorta (2/3 of cases)
• Type B- Descending aorta, distal to left subclavian origin
355.
What is themanagement of Type A aortic
disection?
• Patients with type A aortic dissection should have emergency surgery because of
the high risk of mortality and complication such as aortic regurgitation,
myocardial infarction and cardiac tamponade.
• Surgical management, but blood pressure should be controlled to a target
systolic of 100-120 mmHg whilst awaiting intervention, by IV Labetalol
356.
What are thefeatures of Type A aortic
disection?
• Acute dissection of the ascending aorta can present with complete heart block if
the dissecting haematoma involves the interatrial septum near the
atrioventricular node.
• The combination of chest pain, a (presumed new) diastolic murmur and the ECG
changes make aortic dissection most likely.
357.
What are theinvestigations that you should
do when you suspect Type A aortic disection?
• Transthoracic echocardiogram (TTE) +/- computed tomography (CT) of the thorax
358.
What is themanagement of Type B aortic
disection?
• Most patients with type B dissection should be treated medically unless they
have complications such as persistent leak, rupture or compromised blood flow
to renal, mesenteric or limb circulation.
• Conservative management
• Bed rest
• Decrease blood pressure IV labetalol to prevent progression, if not controlling
you can add Sodium nitroprusside
• endovascular repair of type B aortic dissection may have a role in the future
359.
What are theindications for endovascular
repair in Type B aortic disection?
• Rapidly expanding dissections (>1cm per year)
• Critical diameter (>5.5cm)
• Refractory pain
• Malperfusion syndrome
• Blunt chest trauma
• Penetrating aortic ulcers
360.
What are thediseases that may be associated
with Aortic Disection?
• Hypertension
• Trauma
• Bicuspid aortic valve
• Collagens: marfan's syndrome, ehlers-danlos syndrome
• Turner's and noonan's syndrome
• Pregnancy
• Syphilis
361.
What are theComplications of backward tear
of Aortic Disection?
• Aortic incompetence/regurgitation
• MI: inferior pattern often seen due to right coronary involvement
362.
What are theComplications of forward tear
of Aortic Disection?
• Unequal arm pulses and BP
• Stroke
• Renal failure
363.
The classification ofpulmonary hypertension is currently
changing with the term idiopathic pulmonary arterial
hypertension (IPAH) becoming more widely used, T/F?
• True
364.
What are thecauses of Secondary Pulmonary
Hypertension?
• Secondary causes of pulmonary hypertension include COPD,
congenital heart disease (Eisenmenger's syndrome), recurrent
pulmonary embolism, HIV and sarcoidosis.
365.
What do youknow about Primary pulmonary
hypertension (PPH, now Idiopathic PAH)?
• Pulmonary arterial pressure > 25 mmHg at rest, > 30mmHg with exercise
• PPH is diagnosed when no underlying cause can be found
• Around 10% of cases are familial: autosomal dominant
• Endothelin thought to play a key role in pathogenesis
• Associated with HIV, cocaine and anorexigens (e.g. Fenfluramine)
366.
What are thefeatures of Primary pulmonary
hypertension (PPH, now Idiopathic PAH)?
• More common in females, typically presents at 20-40 years old
• Progressive SOB
• Cyanosis
• Right ventricular heave, loud P2, raised JVP with prominent 'a' waves, tricuspid
regurgitation
367.
What is themanagement of Primary
pulmonary Hypertension?
• Diuretics if right heart failure
• Anticoagulation
• Vasodilator therapy: calcium channel blocker, IV prostaglandins, bosentan:
endothelin-1 receptor antagonist
• Heart-lung transplant
368.
What is PulmonaryArterial Hypertension
(PAH)?
• Pulmonary Arterial Hypertension (PAH) may be defined as a sustained elevation
in mean pulmonary arterial pressure of greater than 25 mmHg at rest or 30
mmHg after exercise.
369.
What are thefeatures of Pulmonary Arterial
Hypertension (PAH)?
• Exertional dyspnea is the most frequent symptom
• Chest pain and syncope may also occur
• Loud P2
• Left parasternal heave (due to right ventricular hypertrophy)
• A pansystolic murmur of tricuspid regurgitation and an early diastolic murmur of
pulmonary insufficiency.
370.
How is Pulmonaryartery hypertension
classified by the WHO?
• Group 1: Pulmonary arterial hypertension (PAH)
• Group 2: Pulmonary hypertension with left heart disease
• Group 3: Pulmonary hypertension secondary to lung disease/hypoxia
• Group 4: Pulmonary hypertension due to thromboembolic disease
• Group 5: Miscellaneous conditions
371.
What are thecauses of Pulmonary Artery Hypertension
that belongs to the WHO classification Group 1:
Pulmonary arterial hypertension (PAH)?
• Idiopathic (previously termed primary pulmonary hypertension)
• Familial
• Associated conditions: collagen vascular disease, congenital heart disease with
systemic to pulmonary shunts, HIV, drugs and toxins, sickle cell disease
• Persistent pulmonary hypertension of the newborn
372.
What are thecauses of Pulmonary Artery Hypertension
that belongs to the WHO classification Group 2:
Pulmonary hypertension with left heart disease?
• left-sided atrial, ventricular or valvular disease such as left ventricular systolic
and diastolic dysfunction, mitral stenosis and mitral regurgitation
373.
What are thecauses of Pulmonary Artery Hypertension that
belongs to the WHO classification Group 3: Pulmonary
hypertension secondary to lung disease/hypoxia ?
• COPD
• Interstitial lung disease
• Sleep apnoea
• High altitude
374.
What are thecauses of Pulmonary Artery Hypertension
that belongs to the WHO classification Group 4:
Pulmonary hypertension due to thromboembolic
disease?
• Sickle cell, Polycythemia ..etc
375.
What are thecauses of Pulmonary Artery Hypertension
that belongs to the WHO classification Group 5:
Miscellaneous conditions
• Lymphangiomatosis e.g. secondary to carcinomatosis or
sarcoidosis
376.
The mechanism bywhich HIV infection produces
pulmonary hypertension remains unknown, T/F?
• True
377.
What is thesingle most important interaction
in case of Pulmonary Artery Hypertension?
• Whilst echocardiography may strongly point towards a diagnosis of pulmonary
hypertension all patients need to have right heart pressures measured.
• Cardiac catheterisation is therefore the single most important
investigation.
378.
What is themanagement of Pulmonary artery
hypertension?
• Management should first involve treating any underlying conditions, for example
with anticoagulants or oxygen.
• Following this, it has now been shown that acute vasodilator testing is central
to deciding on the appropriate management strategy.
• Acute vasodilator testing aims to decide which patients show a significant fall in
pulmonary arterial pressure following the administration of vasodilators such as
intravenous epoprostenol or inhaled nitric oxide
379.
What is themanagement of Pulmonary artery
hypertension if there is a positive response to acute
vasodilator testing?
• If there is a positive response to acute vasodilator testing
• Oral calcium channel blockers
380.
What is themanagement of Pulmonary artery
hypertension if there is a negative response to acute
vasodilator testing?
• If there is a negative response to acute vasodilator testing
• Prostacyclin analogues: treprostinil, ilioprost
• Endothelin receptor antagonists: bosentan
• Phosphodiesterase inhibitors: sildenafil
381.
What is themanagement of Pulmonary artery
hypertension?
• Treatment for pulmonary arterial hypertension is guided by the patients functional
status.
• Patients with class I require no symptomatic treatment while those with class IV
require prostaglanoids, most likely intravenously.
• This patient is short of breath on minimal activity and hence functional class III.
Endothelin receptor antagonists (e.g. bosentan) or phosphodiesterase V inhibitor (e.g.
sildenafil) are appropriate.
• Atrial septostomy and lung transplantation are appropriate for patients who remain
symptomatic at functional class IV despite intravenous prostaglandins and subsequent
combination therapy with bosentan or sildenafil.
382.
What is theproblem of primary pulmonary
hypertension in pregnancy?
• Severe pulmonary hypertension in pregnancy has high mortality
approaching 50%, therefore this patient should be advised about this risk
versus considering a termination.
• Patients who opt against termination of pregnancy should be closely followed up
and managed with anticoagulation, oxygen and pulmonary vasodilator therapy
like prostacyclin.
383.
What are themost common Cyanotic and
Acyanotic Congenital Heart diseases?
• Cyanotic: Transposition of Great Arteries most common at birth, Fallot's most
common overall
• Acyanotic: VSD most common cause
384.
Which is morecommon Tetralogy of or
transposition of the great arteries (TGA)?
• Tetralogy of Fallot is more common than transposition of the great arteries
(TGA), Fallot's doesn't usually present until 1-2 months following the
identification of a murmur or cyanosis.
• In newborn, TGA is the most common presenting cause of cyanotic congenital
heart disease.
385.
What are themost common Acyanotic
Congenital Heart diseases?
• Ventricular septal defects (VSD) - most common, accounts for 30%
• Atrial septal defect (ASD)
• Patent ductus arteriosus (PDA)
• Coarctation of the aorta
• Aortic valve stenosis
• VSDs are more common than ASDs. However, in adult patients ASDs are
the more common new diagnosis as they generally presents later
386.
What are themost common Cyanotic
Congenital Heart diseases?
• Tetralogy of Fallot
• Transposition of the great arteries (TGA)
• Tricuspid atresia
• Pulmonary valve stenosis
387.
Which is morecommon VSD or ASD?
• VSDs are more common than ASDs.
• However, in adult patients ASDs are the more common new diagnosis as they
generally presents later
388.
What is themanagement of post Myocardial
infarction VSD?
• Immediate surgery is recommended whatever the clinical status of the patient.
The most important determinant of early outcome following postinfarction
ventricular septal rupture is the development of heart failure.
• The associated cardiogenic shock leads to end-organ malperfusion, which may be
irreversible.
389.
What is PatentDuctus Arteriosus (PDA)?
• Acyanotic congenital heart defect
• It is a connection between the pulmonary trunk and descending aorta
• more common in premature babies, born at high altitude or maternal rubella
infection in the first trimester
390.
What are thefeatures of Patent Ductus
Arteriosus (PDA)?
• Left subclavicular thrill
• Continuous 'machinery' murmur
• Large volume, collapsing pulse
• Wide pulse pressure
• Heaving apex beat
391.
What is themanagement of Patent Ductus
Arteriosus (PDA)?
• Indomethacin closes the connection in the majority of cases
• If associated with another congenital heart defect amenable to surgery then
prostaglandin E1 is useful to keep the duct open until after surgical repair
392.
What are VentricularSeptal Defects (VSD)?
• Ventricular Septal Defects (VSD) are the most common cause of congenital heart
disease.
• They close spontaneously in around 50% of cases.
• Non-congenital causes include post myocardial infarction
393.
What are thefeatures of Ventricular Septal
Defects (VSD)?
• Classically a pan-systolic murmur which is louder in smaller defects
394.
What are thecomplications of Ventricular
Septal Defects (VSD)?
• Aortic regurgitation (aortic regurgitation is due to a poorly supported right
coronary cusp resulting in cusp prolapsed. AF is associated with ASD)
• Infective endocarditis
• Eisenmenger's complex
• Right heart failure
395.
What is Fickequation?
• In VSD with left to right shunt, the shunt ratio can be calculated using the Fick
equation:
• Qp/Qs = (Ao-Mv)/(PV-PA)
• Where Qp = pulmonary flow, Qs = systemic flow, Ao = aortic saturation, MV =
mixed venous saturation, PV =pulmonary vein saturation (assumed to be 97%)
and PA = pulmonary artery saturation.
396.
According to Fickequation, when should the
decision for surgery in case of VSD be taken?
• When:
• Qp/Qs > 2.0 Surgery for children
• Qp/Qs > 1.5 Surgery for Adult
397.
What are AtrialSeptal Defects (ASDs)?
• Atrial Septal Defects (ASDs) are the most likely congenital heart defect to be
found in adulthood.
• They carry a significant mortality, with 50% of patients being dead at 50 years.
• Two types of ASDs are recognized, ostium secundum and ostium primum.
• Ostium secundum are the most common
398.
What are thefeatures of Atrial Septal Defects
(ASDs)?
• Ejection systolic murmur, fixed splitting of S2
• Embolism may pass from venous system to left side of heart causing a stroke
399.
What are thecomplications of Atrial Septal
Defects (ASDs) in pregnancy?
• Atrial septal defects are usually well tolerated, as pulmonary hypertension is not
usually present at childbearing age.
• However the defect should be closed prior to subsequent pregnancies. In the
presence of Eisenmenger’s syndrome the maternal mortality is approximately
40% and pregnancy is contraindicated, with older maternal age increasing the
risk of pulmonary hypertension and Eisenmenger’s.
400.
What do youknow about Ostium Secundum
Atrial Septal Defects (ASDs)?
• Associated with Holt-Oram syndrome (triphalangeal thumbs)
• ECG: RBBB (Conduction defect) with RAD (Right ventricle is dilated)
(secondum).
401.
What do youknow about Ostium Primum
Atrial Septal Defects (ASDs)?
• Present earlier than ostium secundum defects
• Associated with abnormal AV valves
• ECG: RBBB with LAD, prolonged PR interval
What is Patentforamen ovale (PFO)?
• Patent foramen ovale (PFO) is present in around 20% of the population.
• It may allow embolus (e.g. from DVT) to pass from right side of the heart to the
left side leading to a stroke - 'a paradoxical embolus'. It’s the most common
cause of stroke following DVT.
• There also appears to be an association between migraine and PFO. Some studies
have reported improvement in migraine symptoms following closure of the PFO
404.
How to diagnosePatent Foramen ovale?
• DO TOE (Transesophageal echocardiography)
405.
What is Coarctationof the Aorta ?
• Coarctation of the Aorta describes a congenital narrowing of the descending
aorta, it is more common in females (despite association with Turner's
syndrome).
• Surgical repair is the treatment, but even with repair sometimes recurrence
happen.
406.
What are thefeatures of Coarctation of the
Aorta ?
• Infancy: heart failure
• Adult: hypertension
• Radio-femoral delay
• Mid or late systolic murmur, maximal over back (Thoracic spines)
• Apical click from the aortic valve
• Notching of the inferior border of the ribs (due to collateral vessels) is not seen in
young children
407.
What are thediseases associated with
Coarctation of the Aorta ?
• Turner's syndrome
• Bicuspid aortic valve
• Berry aneurysms
• Neurofibromatosis
• Accelerated Coronary Artesry Disease (CAD)
408.
What is Eisenmenger'sSyndrome?
• Eisenmenger's Syndrome is characterized by the reversal of the left-right shunt
due to pulmonary hypertension.
• The original murmur may disappear once Eisenmenger's syndrome develops.
409.
What are thediseases associated with
Eisenmenger's Syndrome?
• VSD
• ASD
• PDA
410.
What are thefeatures of Eisenmenger's
Syndrome?
• Original murmur may disappear
• Cyanosis
• Clubbing
• Right ventricular failure
• Hemoptysis, embolism
411.
What is themanagement of Eisenmenger's
Syndrome?
• Heart-lung transplantation is required
412.
What do youknow about Bicuspid Aortic Valve?
• Occurs in 1-2% of the population
• Usually asymptomatic in childhood
• The majority eventually develop aortic stenosis or regurgitation
• Associated with a left dominant coronary circulation (the posterior descending
artery arises from the circumflex instead of the right coronary artery) and
turner's syndrome
• Around 5% of patients also have coarctation of the aorta
413.
What are thecomplications of Bicuspid Aortic
Valve?
• Aortic stenosis/regurgitation.
• Higher risk for aortic dissection and aneurysm formation of the
ascending aorta
414.
What is Tetralogyof Fallot (TOF)?
• Tetralogy of Fallot (TOF) is the most common cause of cyanotic congenital heart
disease.
• It typically presents at around 1-2 months, although may not be picked up until
the baby is 6 months old
415.
What are Thefour characteristic features of
Tetralogy of Fallot (TOF)?
• Ventricular septal defect (VSD)
• Right ventricular hypertrophy
• Right ventricular outflow tract (RVOT) obstruction, pulmonary stenosis (The
severity of RVOT obstruction determines the degree of cyanosis and severity)
• Overriding aorta (Aorta that’s connected to both left and right ventricles)
416.
What are theclinical features of Tetralogy of
Fallot (TOF)?
• Cyanosis
• Causes a right-to-left shunt
• Ejection systolic murmur due to pulmonary stenosis (the VSD doesn't usually
cause a murmur)
• A right-sided aortic arch is seen in 25% of patients
• Chest x-ray shows a 'boot-shaped' heart, ECG shows right ventricular hypertrophy
417.
At birth transpositionof the great arteries is the more
common lesion as patients with TOF generally present
at around 1-2 months, T/F?
• True
418.
What is themanagement of Tetralogy of
Fallot (TOF)?
• Surgical repair is often undertaken in two parts
• Cyanotic episodes may be helped by Beta-blockers to decrease infundibular
spasm
419.
What is Dextrocardia?
•Dextrocardia: is a rare condition and occurs with in frequency in
males more than females.
420.
What are theECG features in a patient with
Dextrocardia?
• Classical ECG features:
• Inverted P in lead I
• Shift of the P axis (usually about +120 degrees) and reversed R wave progression.
• Reverse placement of the praecordial leads on the right chest at sites
corresponding to the left chest positions corrects this trend.
421.
What is theprognosis of patient with
Dextrocardia?
• Typically patients have a normal life expectancy if no cardiac
anomalies are present.
422.
A 60-year-old man'sechocardiogram shows a dilated left
ventricular (LV) cavity with the remainder of the other
chamber sizes normal. What is the most likely diagnosis?
• Aortic regurgitation
• Hypertension will cause hypertrophy (increase in muscle) but the
cavity will remain the same
423.
After Cardioversion ofAF, which drug should
be used?
• Amiodarone has been shown to be superior in maintaining sinus rhythm
following DC cardioversion of AF, however, it is associated with more toxic side
effects than the other agents mentioned
424.
What is thetreatment of Malignant Hypertension with
papilloedema, convulsions and pulmonary oedema?
• This constitutes a medical emergency, with IV sodium nitroprusside being the
treatment of choice.
425.
What is themost common cause for flash pulmonary
oedema?
• The most common cause of flash pulmonary oedema is myocardial
ischaemia.
426.
A patient hasNYHA grade II heart failure and is already
receiving angiotensin converting enzyme (ACE)
inhibitors and diuretics, which drug may improve his
survival?
• Beta Blocker
427.
How to treatSupra-Ventricular Tachycardia
associated with pregnancy?
• Regarding the termination of acute SVT, adenosine appears to be safe in
pregnancy.
• In the case of the prevention of recurrent SVT then verapamil or beta-blockers
have data supporting their use.
• Current AHA/EHA criteria for the treatment of SVTs in pregnancy do suggest
using metoprolol (level of evidence 1B) rather than verapamil (C), although they
recommend avoiding the former in the first trimester.
428.
What is acommon cause of
Hypomagnesaemia with Hypertension?
• Diuretic therapy is a common cause of hypomagnesaemia due to increased renal
excretion.
• It is not seen in hyperparathyroidism.
429.
Why MI maybe a result of aortic disection?
• The ECG changes of inferior myocardial infarct suggest that the aneurysm has
dissected the right coronary artery at its ascending aortic ostium.
430.
Why is itimportant to differentiate between
patients with infarction that resulted from
Aortic dissection and that resulted from
Thrombus?
• Thrombolysis will kill a patient with an aortic dissection
431.
What is thedifference between chest pain with
different blood pressure in either arm resulting from
Aortic Aneurysm and Coarctation?
• Coarctation can give different blood pressures in either arm but is a
chronic condition.
432.
In Mitral StenosisThe opening snap is characteristically
lost with heavy valvular calcification, T/F?
• True
433.
The presence ofa small pericardial effusion on echo is
quite common and in this patient who otherwise
appears well, no further action is required, T/F?
• True
434.
In Mitral stenosis, the opening snip is
indicative that the valve is still mobile, T/F?
• True
• Features of mitral stenosis include the loud first heart sound, opening snap and if
in sinus rhythm, a pre-systolic accentuation
435.
Which Hormone willcause immediate rise in
Blood pressure when infused ?
• Angiotensin II when infused intravenously produces an immediate
rise in blood pressure being a potent vasoconstrictor.
436.
Give a methodto calculate ejection fraction using
echocardiography findings?
• One way of measuring ejection fraction is estimated by the ratio between the M-
mode readings of the left ventricular end diastolic diameter divided by the end
systolic diameter.
437.
When we havearrhythmia that’s resulted
from Hyperkalemia, what should we do?
• cardio protection with calcium chloride or gluconate should be first priority and
lowering potassium levels immediately thereafter.
438.
What is theeffect of calcium on
Hyperkalemia?
• Calcium antagonises the effects of hyperkalaemia on a cellular level by a number
of mechanisms.
• These all return myocyte excitability to normal thereby reducing the risk of
arrhythmias.
• Calcium gluconate is the preferred preparation, but calcium chloride can be used.
• Caution is needed if the patient is taking digoxin, as hypercalcaemia can
potentiate its toxicity. The effects of intravenous calcium occur within one to
three minutes but last for only 30-60 minutes, and therefore more definitive
treatment is needed to lower potassium levels.
439.
When we havearrhythmia that’s resulted
from Hyperkalemia, what should we do after
administering calcium?
• Calcium antagonises the effects of hyperkalaemia on a cellular level
• After calcium is given, treatment is required to shift potassium intracellularly. Insulin is most
commonly used, which stimulates the Na-K ATPase pump. The effect is seen within 10-20 minutes
and usually decreases potassium levels by 0.6-1mEq/L. Salbutamol can also increase the action of
the Na-K ATPase pump.
• Sodium bicarbonate infusion can shift potassium intracellularly by increasing blood pH, but its use
is controversial. It is therefore reserved for cases of severe acidosis, or where there is another
indication for its use
440.
What is Remnanthyperlipidaemia (type III
hyperlipidaemia)?
• Remnant hyperlipidaemia is due to abnormal function of the ApoE receptor, which is
normally required for clearance of chylomicron remnants and IDL from the circulation.
• Palmar xanthomas are pathognomonic
• The receptor defect causes levels of chylomicron remnants and IDL to be higher than
normal in the blood stream.
• The receptor defect is an autosomal recessive mutation or polymorphism.The
genotype of the homozygous condition is apo E-2/E-2 and occurs with a frequency of
1:100.
441.
What are thefeatures of Remnant
hyperlipidaemia (type III hyperlipidaemia)?
• Hypercholesterolaemia, typically 8-12 mmol/L
• Hypertriglyceridaemia, typically 5-20 mmol/L
• Normal ApoB concentration
• Palmar xanthomata - orange discoloration of skin creases
• Tuberoeruptive xanthomata - elbows and knees
• Early onset of cardiovascular disease
• Early onset of peripheral vascular disease.
442.
Why Remnant hyperlipidaemia(type III
hyperlipidaemia) is always associated with
another condition that increases lipid?
• Because it is transmitted as an autosomal recessive trait and usually
requires a secondary exacerbating metabolic factor for expression of
the phenotype.
• Therefore, secondary causes of hyperlipidaemia such as hypothyroidism, obesity,
diabetes mellitus, renal insufficiency, high-calorie, high-fat diet or alcohol are
often encountered at diagnosis
443.
Familial hypercholesterolaemia isdue to LDL-receptor
deficiency, and is not associated with elevated
triglyceride levels, T/F?
• True
444.
Which test dowe use to diagnose Patent
Foramen Ovale?
• PFO is then diagnosed by the bubble test – injecting agitated
saline intravenously and looking for bubbles crossing to the left heart.
445.
In which caseswould you give a combination
of ACE and ARBs?
• Valsartan is combined with ACE inhibition in the management of
symptomatic heart failure
446.
What is thetreatment of pulmonary oedema
resulting from Acute mountain sickness?
• Acetazolamide may be of some value in prophylaxis in preventing acute
mountain sickness, but the best prevention is slow acclimatisation.
• High flow oxygen is first line
• Nifedipine reduces pulmonary hypertension and is the treatment of choice for
pulmonary oedema in cases where highflow oxygen is not available.
447.
What is thetreatment of cerebral oedema
resulting from Acute mountain sickness?
• Acetazolamide may be of some value in prophylaxis in preventing acute
mountain sickness, but the best prevention is slow acclimatisation.
• Dexamethasone is the treatment of choice when it occurs
448.
What is Sicksinus syndrome?
• Sick sinus syndrome (SSS), also called sinus node dysfunction (SND), or sinoatrial
node disease, is a group of abnormal heart rhythms (arrhythmias) presumably
caused by a malfunction of the sinus node, the heart's primary pacemaker.
• Bradycardia-tachycardia syndrome is a variant of sick sinus syndrome in which
slow arrhythmias and fast arrhythmias alternate. It is often associated with
ischaemic heart disease and heart valve disease.
449.
What is themanagement of Sick sinus
syndrome?
• Anti-arrhythmics are likely to exacerbate any bradycardia and the
treatment of choice would be a permanent pacemaker.
• Dual chamber pacemakers are usually used, as single chamber pacing
may be associated with the development of ‘pacemaker syndrome’.
450.
What are theECG appearances that are
compatible with a pericardial effusion?
• The ECG obtained from the patient is of low voltage and shows QRS
complexes of alternating amplitude (electrical Alternans) and sinus
tachycardia.
451.
A patient postMI shows immediate signs of ventricular
tachycardia VS another patients who presents with
Vtach a month later, what is the difference in
management?
• The development of ventricular tachycardia/fibrillation (VT/VF) in the first day
following an acute myocardial infarction (MI) is thought to be of no prognostic
significance if dealt with promptly.
• However the late development of VT/VF in the context of a full thickness myocardial
scar, as evidenced by the Q waves on the electrocardiogram (ECG), carries a very poor
prognosis.
• Implantable defibrillators have been shown to offer improved survival over anti-
arrhythmic therapy.
• Amiodarone would be an appropriate choice in patients unsuitable for defibrillator
insertion.
452.
How can youdiagnose Accelerated
hypertension using fundoscopy?
• evidenced by the fundoscopic findings of Grade III retinopathy
453.
What is themanagement of accelerated
hypertension?
• Patients with accelerated hypertension should be admitted to hospital for
initiation of antihypertensive medication and regular blood pressure
monitoring.
• Initial treatment can be with ORAL nifedipine or atenolol, escalating to
intravenous therapy with nitrates if there is no effect.
• Sublingual nifedipine should be avoided as it might lead to a sudden drop in
blood pressure, which could interfere with the autoregulatory mechanism of
cerebral perfusion leading to an ischaemic stroke.
454.
What are thefeatures of carotid sinus
hypersensitivity?
• carotid sinus hypersensitivity (CSH), demonstrating an exaggerated response to
carotid sinus stimulation.
• The diagnosis is only made after ischaemic heart disease or rhythm disturbance
have been reasonably excluded, as in this case.
• CSH may be predominantly cardioinhibitory (resulting in bradycardia),
vasodilatory (resulting in hypotension), or a mixture of the two.
455.
What is themanagement of carotid sinus
hypersensitivity?
• Cardioinhibitory CSH is usually managed with insertion of a dual-chamber
pacemaker, and vasodilatory CSH is managed with support stockings,
fludrocortisone and midodrine (available on a named-patient basis in the UK).
456.
What is Tocolysis-associatedpulmonary
oedema?
• Tocolytics are medications administered for the suppression of premature
contractions. Acute pulmonary oedema can occur with administration of β2
agonists for tocolysis in up to 5–15% of cases.
• It usually occurs after 24 h of administration of these agents. The chest X-ray
reveals pulmonary infiltrates and normal heart size.
• Concomitant use of corticosteroids that are often administered for lung
maturation have also been implicated as risk factor for development of tocolysis-
associated pulmonary oedema.
• Treatment involves stopping the tocolytics, oxygen and careful volume control.
457.
What is theleading causes of death following
acute myocardial infarction?
• Autopsy studies reveal that ventricular free wall rupture occurs about 10
times more frequently than pos-tinfarction ventricular septal rupture, occurring
in about 11% of patients following acute myocardial infarction.
• Ventricular rupture and cardiogenic shock are now the leading causes of death
following acute myocardial infarction, and together account for over two-thirds
of early deaths in patients suffering their first acute infarction.
458.
What are thefeatures and management of
Cardiac Tamponade, following ventricular wall
rapture after Myocardial infarction?
• Sudden onset of breathlessness with clear lung fields, cardiogenic shock and
electrical alternans, consistent with ventricular rupture.
• In this case the patient is shocked and needs haemodynamic support, but the
definitive treatment is drainage of the pericardial sac with emergency
ventricular repair.
• An aortic balloon pump is often used in conjunction with inotropes and colloid
replacement to stabilise the patient before a pericardiocentesis takes place.
459.
What is themanagement of acute right ventricular
failure occurring after right ventricular Myocardial
infarction?
• Therapy for hypotension associated with RVMI involves boluses of iv saline to
improve right ventricular (RV) preload and cardiac output.
• If up to 1.5 l of normal saline does not correct hypotension, invasive
haemodynamic monitoring should be considered to guide further fluid therapy.
• Similarly inotropic support may be considered after adequate fluid resuscitation
has failed.
• Furosemide will reduce RV filling pressure and should be avoided
460.
What is themanagement of a patient who did
stenting after myocardial infarction, then two days
he presented with symptoms of another MI?
• Another myocardial infarction in the same vascular territory two days after intra-coronary
stenting suggests stent thrombosis in this patient.
• Stent thrombosis usually occurs in the first two days after the procedure.
• Combined antiplatelet therapy with aspirin and clopidogrel, reduces the risk of thrombosis
• This patient should be taken immediately to the Cardiac Catheterisation Lab with a view to
performing angioplasty or to administer intracoronary thrombolytic therapy to open up the
blocked stent.
• Simultaneous use of abciximab (a glycoprotein IIb/IIIa inhibitor) has been shown to improve
morbidity and mortality in acute coronary stent thrombosis
461.
What is themanagement of Cardiogenic
shock developed after Myocardial infarction?
• Cardiogenic shock occurs in about 7% of cases of acute myocardial infarction; of
these 10% have this condition at admission and 90% develop it in hospital; it
carries high mortality.
• Management of cardiogenic shock in this setting involves circulatory support in
the form of vasopressors such as IV dopamine and intraaortic balloon pump
(IABP).
462.
A patient missesa dose of warfarin, what
should she do?
• Warfarin should be taken about the same time each day.
• If she forgot to take her warfarin, she could take it later that day.
• If she forgot to take it one day, she should not take a double dose the next day,
she should just continue with the regular dose
463.
What is pacemakersyndrome?
• The VVIR prefix denotes a single Ventricular lead pacemaker, which senses and
paces the Ventricle and Inhibits Responses to a sensed event.
• An untimely contraction of the atria caused by retrograde conduction of the
ventricular pacemaker impulse mimics complete heart block and the pounding
is the feeling of atria contracting against a closed tricuspid valve causing cannon
waves in the neck.
• The treatment is to upgrade the system to a dual chamber pacemaker; this
allows the atria to sense any retrograde electrical impulse, so inhibiting native
atrial depolarisation.
464.
What is Takasubocardiomyopathy?
• This is a patient with cardiac sounding chest pain with a troponin positive event, in
the absence of vascular risk factors, and in the context of normal coronary vessels.
• The diagnosis is made on the LV description: apical ballooning is pathopneumonic of
Takasubo cardiomyopathy, with the shape of the heart named after the Japanese
octopus trap.
• It classically presents in post-menopausal women, and is particularly triggered by
anxiety and emotional stress. Treatment is supportive as per heart failure, possibly
requiring inotropes if there is no LV outflow tract obstruction and with beta blockade
if there is LV outflow tract obstruction. Patients generally recover their LV ejection
fraction within 4 weeks.
465.
What is therelationship between cisplatin
and AF?
• A common side effect of cisplatin is hypomagnesaemia which can result in
muscle cramps, tremor, cardiac arrhythmias, confusion amongst other
features.
466.
What is Atrialflutter?
• Atrial flutter is a form of supraventricular tachycardia characterised by a
succession of rapid atrial depolarisation waves.
• ECG findings
• 'sawtooth' appearance
• as the underlying atrial rate is often around 300/min the ventricular or heart rate is
dependent on the degree of AV block. For example if there is 2:1 block the ventricular rate
will be 150/min
• flutter waves may be visible following carotid sinus massage or adenosine
467.
What is themanagement of Atrial flutter?
• is similar to that of atrial fibrillation although mediction may be less effective
• atrial flutter is more sensitive to cardioversion however so lower energy levels
may be used
• radiofrequency ablation of the tricuspid valve isthmus is curative for most
patients
468.
What is Ranolazine?
•Ranolazine is a viable option in the management of angina where other avenues
have been exhausted.
• It works by inhibiting the delayed sodium influx channel in the myocardium,
reducing the intracellular calcium concentrations in the heart muscle.
• This in turn leads to a negative inotropic effect and reduction in symptoms of
angina.
• Ranolazine does not cause a profound hypotensive effect
469.
What is apathological q?
• The older and simpler definition of a pathological Q wave:
Q-wave of >=0.04 s and an amplitude >=25% of the R-wave in that lead
470.
What are Stokes-Adamsattacks?
• Stokes Adams attack: Sudden collapse into unconsciousness due to a disorder of
heart rhythm in which there is a slow or absent pulse resulting in syncope
(fainting) with or without convulsions.
• In this condition, the normal heartbeat passing from the upper chambers of the
heart to the lower chambers is interrupted. This results in a condition called a
"heart block." When a heart block occurs, the heart rate usually slows
considerably. This can cause inadequate blood flow to the brain and result in
fainting.
471.
What is Earlyrepolarization variant?
• There exists a benign but often alarming electrocardiographic entity that presents with ST
segment elevation.
• It is known as the early repolarization variant and expresses as an early uptake of the ST segment
before the descending limb of the R wave has reached the baseline. Features of early
repolarization variant are:
• Classically the ST segment elevation during exercise returns to the baseline following cessation of
exercise
• It is common in black males
• Clinical evaluation is entirely normal
• ST elevation is usually seen in the precordial leads
472.
When you havea patient presenting with malignant
hypertension, should you give IV nitroprosside or Oral
Captopril?
• IV sodium nitroprusside titrated for gradual BP reduction would be a good
choice.
• IV labetolol may be a reasonable alrernative.
• Sublingual nifedipine and oral captopril would cause rapid BP reduction followed
by rebound in blood pressure and may be associated with increased mortality
although the evidence to support this notion is a little weak.
473.
A patient whodeveloped ventricular fibrillation due to
severe hypothermia (below 30 degree), can you give
him drugs or DC shock ?
• At core temperatures of less than 30°C, treatment of ventricular arrhythmias
with medical therapy is largely ineffective and electrical cardioversion is less
effective.
• For this reason, a prolonged period of CPR may be required until core
temperature is above 30ºC.
474.
What is themanagement of acute respiratory
distress syndrome (ARDS)?
• Initial resuscitation should involve high flow oxygen and intravenous (iv) fluids to
maintain high right ventricular filling pressures (Opposite of cardiogenic
pulmonary edema) . Steroid therapy is normally introduced later in ARDS, used at
this stage it can worsen pulmonary oedema, and evidence is equivocal as to
benefit.
• Continuous positive airways pressure ventilation would help in the management
of the pulmonary oedema and is the next consideration after IV fluids. It should
be noted that diuretic treatment would be strongly contraindicated in this case.
This is because right ventricular output is dependent on elevated filling
What are theindications of Intra Aortic
balloon pump?
477.
You have apatient that you want to know if
he Is getting ischemia with exercise, should
you do Thalium or PC angiography?
• Diagnostic angiography provides angiographic detail of coronary
anatomy but will not provide functional information.
• Thallium perfusion scanning and myocardial contrast perfusion
echocardiography are all capable of localising ischaemia.
478.
What is Cardiacindex?
• Cardiac index (CI) is a haemodynamic parameter that relates the cardiac output
(CO) from left ventricle in one minute to body surface area (BSA), thus relating
heart performance to the size of the individual. The unit of measurement is litres
per minute per square metre (L/min/m2
).
• The normal range of cardiac index in rest is 2.6–4.2 L/min/m2
.
479.
What is theuse of Hyponatremia as a
prognostic factor for congestive heart failure?
• Non-iatrogenic hyponatraemia in the context of congestive cardiac
failure carries a poor prognosis as it is secondary to significant fluid
overload.
• It was thought that specific vasopressin antagonists may offer a
significant prognostic advantage in patients with heart failure and
marked hyponatraemia, but the data so far have proved very
disappointing.
480.
Why Cyclizine iscontraindicated to be given
after MI?
• Cyclizine is a H1 receptor antagonist and anticholinergic, resulting in systemic
hypertension and inducing tachycardia.
• It can aggravate a fragile myocardium into acute failure and is hence not
recommended by NICE in patients with ACS or severe heart failure1.