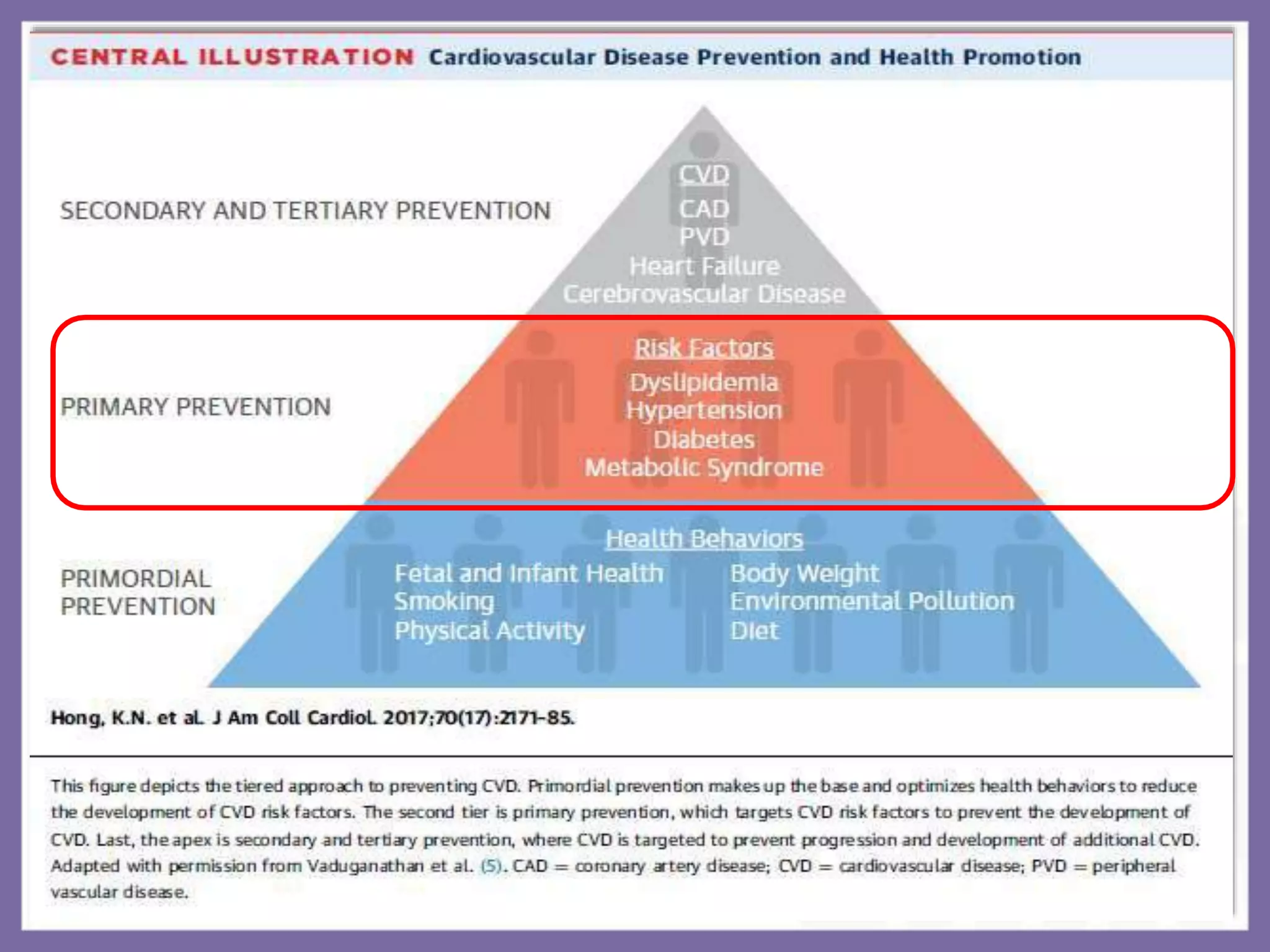
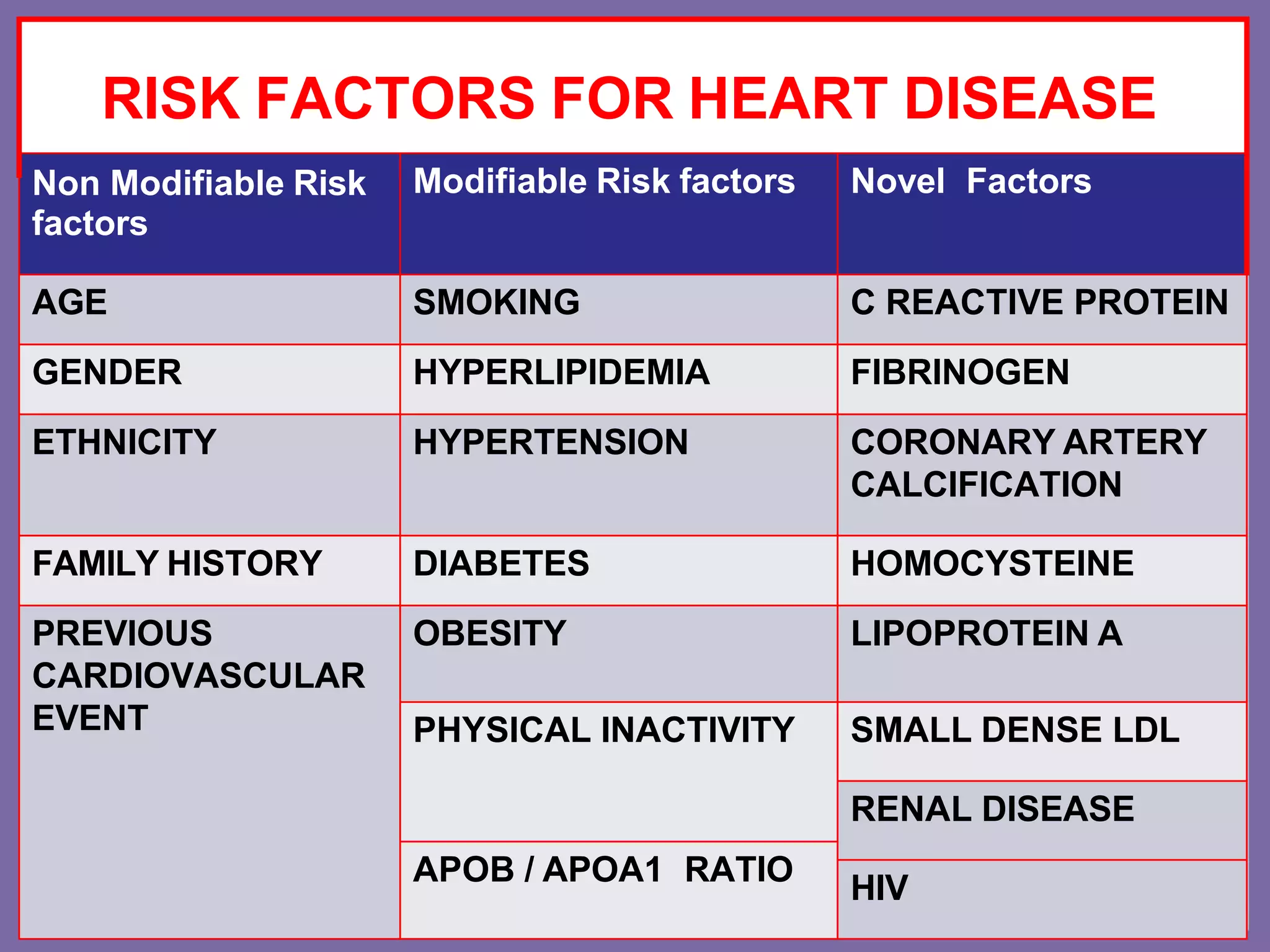
Primary prevention aims to avert disease onset by addressing risk factors for coronary artery disease (CAD) through tailored therapies and lifestyle changes. Key risk factors include smoking, hypertension, obesity, and diabetes, with particular emphasis on the detrimental effects of smoking and the complexity of hypertension's impact on heart health. Effective management strategies include lifestyle modifications, regular screenings, and medication where appropriate, focusing on comprehensive approaches to reduce CAD risk.