ca colorectal powerpoint explanation inn
•Download as PPTX, PDF•
0 likes•3 views
penjelasan mengenai kanker kolorektal
Report
Share
Report
Share

Recommended
Esophagectomy
This document discusses surgical approaches for esophageal cancer. It covers:
- Esophageal anatomy, blood supply, lymph drainage
- Staging of esophageal cancer and criteria for resection
- Preoperative evaluation including imaging, biopsy, and laparoscopy
- Surgical procedures for cervical, thoracic, and esophagogastric junction cancers including transhiatal esophagectomy, Ivor-Lewis procedure, and tri-incisional esophagectomy
- Oncologic principles for lymphadenectomy and margins during resection
Metastatic colorectal liver cancer
This document discusses metastatic colorectal liver cancer. It outlines risk factors, evaluation, and treatment options including surgery, chemotherapy, local tumor ablation, and radiotherapy. Surgery offers the best chance of survival if metastases are resectable, with 5-year survival rates of 24-58% for resection. Neoadjuvant chemotherapy can help make previously unresectable tumors operable. Local ablation techniques are alternatives for tumors that cannot be surgically removed.
Esophagectomy : APPROACHES, CONTROVERSIES AND CURRENT EVIDENCE
This document discusses esophagectomy, the surgical approaches for esophageal cancer resection. It covers the relevant anatomy, blood supply, lymph drainage, and histology of esophageal cancer. It then discusses pre-treatment evaluation including staging assessments and criteria for resection. The key surgical procedures for cervical, thoracic, and esophagogastric junction cancers are described including the transhiatal, Ivor-Lewis, and tri-incisional approaches. Post-operative outcomes from recent studies comparing these approaches are summarized.
Colo rectal carcinoma
This document provides an overview of colorectal carcinoma, including its anatomy, genetics, risk factors, screening, diagnosis, staging, and treatment strategies. Some key points:
- Colorectal cancer is one of the most common cancers worldwide. Proximal colon cancer is usually related to microsatellite instability, while distal colon cancer is associated with chromosomal instability.
- Risk factors include diet, smoking, inflammation. Screening includes fecal occult blood tests and endoscopy starting at age 50.
- Staging involves examining tumor depth, lymph node involvement, and metastasis. Treatment depends on stage but generally involves surgical resection with or without chemotherapy or radiation. The goal is sphincter preservation for rectal cancers
Esophageal carcinoma
Benign tumors of the esophagus include leiomyomas, cysts, and polyps. Leiomyomas are the most common benign tumor, usually occurring in the lower two-thirds of the esophagus in males. Esophageal cysts often present in childhood and are located along the right side. Malignant esophageal tumors are usually advanced at diagnosis and involve the muscular wall. Squamous cell carcinoma is most common and risk factors include smoking and alcohol. Diagnosis involves endoscopy with biopsy and imaging such as CT scan. Treatment options include surgery, chemotherapy, and radiation, but long-term survival remains low given late-stage presentation.
Colorectal cancer.pptx by -MANOJIT(MS)
Colon cancer is the second most common cancer and most common gastrointestinal malignancy. It typically presents between ages 45-65. The predominant type is adenocarcinoma. Risk factors include family history, inflammatory bowel disease, and diet low in fruits and vegetables. Treatment involves surgical resection of the primary tumor with or without chemotherapy depending on staging. Palliative options are considered for metastatic or unresectable disease.
Gastric carcinoma
This document summarizes information about gastric carcinoma (stomach cancer). It covers the epidemiology, anatomy, pathology, risk factors, clinical presentation, staging, and treatment of gastric cancer. Key points include:
- Gastric cancer was previously a leading cause of cancer death but now ranks fourth most common. Incidence is highest in China and Japan.
- The stomach has extensive lymphatic drainage involving 16 lymph node stations.
- 95% of gastric cancers are adenocarcinomas. Other rare types include squamous cell carcinoma and carcinoid tumors.
- Risk factors include smoking, obesity, and H. pylori infection. Symptoms are often vague but may include weight loss, abdominal pain,
Recommended
Esophagectomy
This document discusses surgical approaches for esophageal cancer. It covers:
- Esophageal anatomy, blood supply, lymph drainage
- Staging of esophageal cancer and criteria for resection
- Preoperative evaluation including imaging, biopsy, and laparoscopy
- Surgical procedures for cervical, thoracic, and esophagogastric junction cancers including transhiatal esophagectomy, Ivor-Lewis procedure, and tri-incisional esophagectomy
- Oncologic principles for lymphadenectomy and margins during resection
Metastatic colorectal liver cancer
This document discusses metastatic colorectal liver cancer. It outlines risk factors, evaluation, and treatment options including surgery, chemotherapy, local tumor ablation, and radiotherapy. Surgery offers the best chance of survival if metastases are resectable, with 5-year survival rates of 24-58% for resection. Neoadjuvant chemotherapy can help make previously unresectable tumors operable. Local ablation techniques are alternatives for tumors that cannot be surgically removed.
Esophagectomy : APPROACHES, CONTROVERSIES AND CURRENT EVIDENCE
This document discusses esophagectomy, the surgical approaches for esophageal cancer resection. It covers the relevant anatomy, blood supply, lymph drainage, and histology of esophageal cancer. It then discusses pre-treatment evaluation including staging assessments and criteria for resection. The key surgical procedures for cervical, thoracic, and esophagogastric junction cancers are described including the transhiatal, Ivor-Lewis, and tri-incisional approaches. Post-operative outcomes from recent studies comparing these approaches are summarized.
Colo rectal carcinoma
This document provides an overview of colorectal carcinoma, including its anatomy, genetics, risk factors, screening, diagnosis, staging, and treatment strategies. Some key points:
- Colorectal cancer is one of the most common cancers worldwide. Proximal colon cancer is usually related to microsatellite instability, while distal colon cancer is associated with chromosomal instability.
- Risk factors include diet, smoking, inflammation. Screening includes fecal occult blood tests and endoscopy starting at age 50.
- Staging involves examining tumor depth, lymph node involvement, and metastasis. Treatment depends on stage but generally involves surgical resection with or without chemotherapy or radiation. The goal is sphincter preservation for rectal cancers
Esophageal carcinoma
Benign tumors of the esophagus include leiomyomas, cysts, and polyps. Leiomyomas are the most common benign tumor, usually occurring in the lower two-thirds of the esophagus in males. Esophageal cysts often present in childhood and are located along the right side. Malignant esophageal tumors are usually advanced at diagnosis and involve the muscular wall. Squamous cell carcinoma is most common and risk factors include smoking and alcohol. Diagnosis involves endoscopy with biopsy and imaging such as CT scan. Treatment options include surgery, chemotherapy, and radiation, but long-term survival remains low given late-stage presentation.
Colorectal cancer.pptx by -MANOJIT(MS)
Colon cancer is the second most common cancer and most common gastrointestinal malignancy. It typically presents between ages 45-65. The predominant type is adenocarcinoma. Risk factors include family history, inflammatory bowel disease, and diet low in fruits and vegetables. Treatment involves surgical resection of the primary tumor with or without chemotherapy depending on staging. Palliative options are considered for metastatic or unresectable disease.
Gastric carcinoma
This document summarizes information about gastric carcinoma (stomach cancer). It covers the epidemiology, anatomy, pathology, risk factors, clinical presentation, staging, and treatment of gastric cancer. Key points include:
- Gastric cancer was previously a leading cause of cancer death but now ranks fourth most common. Incidence is highest in China and Japan.
- The stomach has extensive lymphatic drainage involving 16 lymph node stations.
- 95% of gastric cancers are adenocarcinomas. Other rare types include squamous cell carcinoma and carcinoid tumors.
- Risk factors include smoking, obesity, and H. pylori infection. Symptoms are often vague but may include weight loss, abdominal pain,
management of pancreatic cancer.pptx
1) Chemotherapy alone is the preferred adjuvant treatment after surgical resection of pancreatic cancer based on multiple trials showing a survival benefit. 2) Some trials showed improved survival with the addition of chemoradiotherapy to chemotherapy compared to chemotherapy alone, though the benefit is unclear. 3) Optimal chemotherapy regimens may include gemcitabine, gemcitabine plus capecitabine, FOLFIRINOX, or gemcitabine plus nab-paclitaxel based on various trial results.
Regional therapy for tumors 2
Regional therapy options for tumors include embolization (bland, chemo, radio) and ablation (radiofrequency, cryo). Embolization is useful for colorectal cancer, hepatocellular carcinoma, cholangiocarcinoma, and neuroendocrine metastases. Chemoembolization is palliative for primary and metastatic liver cancer. It provides a survival benefit compared to best supportive care alone in salvage patients. Radioembolization also prolongs survival compared to supportive care. Transarterial chemoembolization improves survival for unresectable cholangiocarcinoma and hepatocellular carcinoma compared to systemic therapy or supportive care alone.
A complete gallbladder cancer review.pptx
Gallbladder cancer is a relatively rare but aggressive form of cancer. The 5-year survival rate is only 20% overall but can reach 65% for localized cancers that are surgically resected. Risk factors include gallstone disease and gallbladder polyps. Symptoms often include pain, jaundice, weight loss and fatigue. Diagnosis involves blood tests, ultrasound, CT/MRI and biopsy. Surgical resection offers the best chance of cure for early stage disease while chemotherapy and radiation are used for advanced or metastatic cancers. Prognosis depends highly on stage, with 5-year survival rates of 100%, 65-80%, 30-70%, and less than 15% for stages I through IV, respectively.
Gall bladder carcinoma
Gall bladder carcinoma seen in Indian popluation most common in women and presents at a very late stage .Survival is in months hence palliative treatment is being preferred .
Carcinoma of esophagus
This document discusses esophageal cancer, including:
- It remains the 6th most common malignancy and rates vary globally. Squamous cell carcinoma is most common.
- Risk factors include smoking, alcohol, hot liquids and micronutrient deficiencies. Barrett's esophagus increases adenocarcinoma risk.
- Symptoms depend on location and stage but include dysphagia, weight loss, pain and cough.
- Diagnostic tools include endoscopy, CT, PET, MRI and EUS to determine stage.
- Treatment involves chemotherapy, radiation, and surgery depending on location and stage. Surgical techniques include transhiatal, Ivor Lewis and minimally invasive approaches.
Colorectal liver metastases multidisciplinary approach 2 (2)
This document discusses treatment options for colorectal liver metastases. It summarizes that resection provides the best chance for long-term survival, with 5-year survival rates of 45-60%. Radiofrequency ablation can treat small, unresectable tumors but does not replace resection. While chemotherapy provides a median survival of 14.5 months, combining chemotherapy with resection can yield 5-year survival of 37-58%. The document discusses various approaches for increasing resectability and managing synchronous primary and metastatic tumors. It emphasizes the importance of a multidisciplinary team approach at high-volume centers for optimal outcomes.
Colorectal liver metastases multidisciplinary approach 2 (2)
This document discusses treatment options for colorectal liver metastases. It summarizes that resection provides the best chance for long-term survival, with 5-year survival rates of 45-60%. Radiofrequency ablation can treat small, unresectable tumors but does not replace resection. For resectable tumors, options include chemotherapy with or without resection. A multidisciplinary team approach is important for evaluating all treatment possibilities.
Ovary 1
This document discusses the management of ovarian cancer. It covers risk-reducing salpingo-oophorectomy (RRSO) for high-risk patients, surgical staging techniques including open and minimally invasive approaches, management of early-stage disease including adjuvant chemotherapy and radiation, cytoreductive surgery and goals for advanced-stage disease, and the role of interval debulking surgery after neoadjuvant chemotherapy. Complete resection of all tumor is the optimal outcome for advanced ovarian cancer to improve survival outcomes.
management of Liver cancers
This document outlines recent advances in the management of liver cancers. It discusses the epidemiology, risk factors, classification, investigations and various treatment options for liver cancers including hepatic resection, ablation techniques, regional therapies, chemotherapy and transplantation. Resection remains the standard curative treatment for non-cirrhotic patients with localized disease, while ablation techniques and regional therapies are alternatives for patients not eligible for surgery. Advances in surgical techniques and anesthesia have improved resection outcomes.
Carcinoma stomach management
Carcinoma of the stomach is usually suspected based on symptoms like abdominal pain or indigestion. Investigations include endoscopy with biopsy, which is the gold standard for diagnosis. Staging involves endoscopic ultrasound, CT, PET scans and laparoscopy. Treatment depends on the stage, and may involve surgery such as gastrectomy with lymph node dissection, adjuvant chemotherapy and/or radiotherapy. Prognosis depends on factors like stage, lymph node involvement and response to treatment, with 5-year survival rates ranging from 95% for early stage to near 0% for metastatic disease.
Hepatocellular carcinoma 2020
This document provides an overview of the management of hepatocellular carcinoma (HCC). It discusses the epidemiology, risk factors, diagnosis and staging, as well as treatment options for HCC. The major risk factors for HCC include hepatitis B virus, hepatitis C virus, and alcohol. Treatment depends on the stage and includes options such as liver transplantation, resection, ablation, transarterial chemoembolization, and the systemic therapy sorafenib. Prevention through vaccination and treating underlying liver diseases can help reduce cases of HCC.
Rectal cancer alex
1. Rectal cancer is a common malignancy that arises in the rectum, usually within 15 cm of the anal verge.
2. Diagnostic workup includes physical exam, proctoscopy, biopsy of the primary tumor, and imaging. Blood tests like CEA are also done.
3. Treatment involves a multidisciplinary approach with surgery, often total mesorectal excision, along with pre- or post-operative chemoradiation to reduce the risk of recurrence. The type of surgery depends on how far the cancer has spread.
Carcinoma esophagus
This document provides an overview of carcinoma of the esophagus, including epidemiology, etiology, classification, diagnosis, staging, and management. It discusses the different types of esophageal cancer, risk factors, pre-malignant conditions, patterns of spread, diagnostic tools such as endoscopy and imaging, and the AJCC staging system. Treatment options are covered for early stage disease including endoscopic resection and ablation methods, as well as surgical approaches for localized and advanced disease, including transhiatal esophagectomy, Ivor-Lewis esophagectomy, and McKeown esophagectomy. Post-operative complications are also reviewed.
gastriccancer
This document discusses gastric cancer, including its epidemiology, risk factors, diagnosis, treatment, and outcomes. Some key points:
- Gastric cancer is the 4th most common cancer worldwide and the 15th most common in the US. Incidence has declined significantly over the last century.
- Risk factors include H. pylori infection, smoking, diet high in salted/smoked foods, and adenomatous polyps.
- Diagnosis is typically made via endoscopy with biopsy. Staging may involve endoscopic ultrasound, CT scan, or laparoscopy.
- Treatment is usually surgical resection with D1 or D2 lymph node dissection and chemotherapy/radiation. Total or
Rathod Gastric Cancer Presentation final.pptx
- Gastric cancer is the fourth most common cancer worldwide and the second leading cause of cancer death. It is more common in older individuals, males, and those in East Asia. Risk factors include H. pylori infection, dietary factors like salt and smoking, and hereditary conditions.
- Staging workup includes endoscopy with biopsy, EUS, CT, PET, and laparoscopy to determine depth of invasion, lymph node involvement, and metastasis. Surgery is the main treatment and may be combined with chemotherapy or radiation depending on stage. Outcomes have improved with more extensive lymph node dissection and adjuvant therapy. Palliative options exist for advanced or unresectable cases.
Rectal Carcinoma
This document provides an overview of rectal carcinoma. It discusses the epidemiology, risk factors, clinical presentation, investigations, staging, and treatment options. Rectal carcinoma is the third most common cause of cancer deaths in the USA, with over 150,000 new cases diagnosed annually. Treatment may involve local excision, low anterior resection, abdominoperineal resection, or multivisceral resection depending on the stage, size, and location of the tumor. Total mesorectal excision and adjuvant chemoradiation are important to reduce local recurrence rates.
Hcc
1) Surgical management of hepatocellular carcinoma (HCC) in Egypt must be seen in the context of various treatment modalities like resection, transplantation, and interventional radiology which should be used in a complementary rather than exclusive manner.
2) Liver transplantation according to the Milan criteria provides the best oncologic outcomes for HCC but has limitations related to tumor size and number as well as donor availability. Surgical resection remains important for patients outside transplant criteria.
3) Surgical techniques have improved outcomes with resection, including careful patient selection, mapping of lesions, and attention to surgical details to achieve low mortality and recurrence rates. Bridging therapies and downstaging can increase transplant eligibility.
Role of surgery in metastatic colorectal cancer
Surgery plays an important role in treating metastatic colorectal cancer. The document discusses:
1) The liver is the most common site of metastasis and surgical resection of isolated liver metastases can provide a 5-year survival rate of 45-60%, compared to just 6-9 months with no treatment.
2) Other potentially resectable isolated metastases, such as those in the lungs or peritoneum, may also be treated with surgery, providing 5-year survival rates around 20-40%.
3) Neoadjuvant chemotherapy can downsize initially unresectable liver metastases to make them resectable and improve long-term outcomes compared to surgery alone.
pancreatic cas managementby bedrumoh.pptx
1. Pancreatic cancer is the 4th leading cause of cancer death and often presents with jaundice, abdominal pain, weight loss, or new-onset diabetes. Diagnosis involves blood tests, CT, MRI, EUS, and biopsy.
2. Surgical management includes Whipple procedure for head tumors or distal pancreatectomy for body/tail tumors. Palliative options relieve biliary/duodenal obstruction and pain via stenting, bypass, or celiac plexus block.
3. Adjuvant chemo-radiotherapy after surgery can increase survival compared to surgery alone. Neoadjuvant FOLFIRINOX increases resectability of borderline resect
Management of Carcinoma Rectum.pptx
- Management of rectal cancer has changed dramatically in recent decades with multimodality treatment becoming standard.
- Surgery remains the primary treatment but local recurrence rates were historically high at 20-50% with surgery alone.
- Total mesorectal excision has significantly reduced local recurrence rates by completely removing the mesorectum containing the tumor and draining lymph nodes.
- Adjuvant chemoradiation or neoadjuvant chemoradiation further lower recurrence rates and improve survival compared to surgery alone.
Identification and nursing management of congenital malformations .pptx
Identification and nursing management of congenital malformations .pptxMGM SCHOOL/COLLEGE OF NURSING
Identification and nursing management of congenital malformations ABDOMINAL TRAUMA in pediatrics part one.
Abdominal trauma in pediatrics refers to injuries or damage to the abdominal organs in children. It can occur due to various causes such as falls, motor vehicle accidents, sports-related injuries, and physical abuse. Children are more vulnerable to abdominal trauma due to their unique anatomical and physiological characteristics. Signs and symptoms include abdominal pain, tenderness, distension, vomiting, and signs of shock. Diagnosis involves physical examination, imaging studies, and laboratory tests. Management depends on the severity and may involve conservative treatment or surgical intervention. Prevention is crucial in reducing the incidence of abdominal trauma in children.
More Related Content
Similar to ca colorectal powerpoint explanation inn
management of pancreatic cancer.pptx
1) Chemotherapy alone is the preferred adjuvant treatment after surgical resection of pancreatic cancer based on multiple trials showing a survival benefit. 2) Some trials showed improved survival with the addition of chemoradiotherapy to chemotherapy compared to chemotherapy alone, though the benefit is unclear. 3) Optimal chemotherapy regimens may include gemcitabine, gemcitabine plus capecitabine, FOLFIRINOX, or gemcitabine plus nab-paclitaxel based on various trial results.
Regional therapy for tumors 2
Regional therapy options for tumors include embolization (bland, chemo, radio) and ablation (radiofrequency, cryo). Embolization is useful for colorectal cancer, hepatocellular carcinoma, cholangiocarcinoma, and neuroendocrine metastases. Chemoembolization is palliative for primary and metastatic liver cancer. It provides a survival benefit compared to best supportive care alone in salvage patients. Radioembolization also prolongs survival compared to supportive care. Transarterial chemoembolization improves survival for unresectable cholangiocarcinoma and hepatocellular carcinoma compared to systemic therapy or supportive care alone.
A complete gallbladder cancer review.pptx
Gallbladder cancer is a relatively rare but aggressive form of cancer. The 5-year survival rate is only 20% overall but can reach 65% for localized cancers that are surgically resected. Risk factors include gallstone disease and gallbladder polyps. Symptoms often include pain, jaundice, weight loss and fatigue. Diagnosis involves blood tests, ultrasound, CT/MRI and biopsy. Surgical resection offers the best chance of cure for early stage disease while chemotherapy and radiation are used for advanced or metastatic cancers. Prognosis depends highly on stage, with 5-year survival rates of 100%, 65-80%, 30-70%, and less than 15% for stages I through IV, respectively.
Gall bladder carcinoma
Gall bladder carcinoma seen in Indian popluation most common in women and presents at a very late stage .Survival is in months hence palliative treatment is being preferred .
Carcinoma of esophagus
This document discusses esophageal cancer, including:
- It remains the 6th most common malignancy and rates vary globally. Squamous cell carcinoma is most common.
- Risk factors include smoking, alcohol, hot liquids and micronutrient deficiencies. Barrett's esophagus increases adenocarcinoma risk.
- Symptoms depend on location and stage but include dysphagia, weight loss, pain and cough.
- Diagnostic tools include endoscopy, CT, PET, MRI and EUS to determine stage.
- Treatment involves chemotherapy, radiation, and surgery depending on location and stage. Surgical techniques include transhiatal, Ivor Lewis and minimally invasive approaches.
Colorectal liver metastases multidisciplinary approach 2 (2)
This document discusses treatment options for colorectal liver metastases. It summarizes that resection provides the best chance for long-term survival, with 5-year survival rates of 45-60%. Radiofrequency ablation can treat small, unresectable tumors but does not replace resection. While chemotherapy provides a median survival of 14.5 months, combining chemotherapy with resection can yield 5-year survival of 37-58%. The document discusses various approaches for increasing resectability and managing synchronous primary and metastatic tumors. It emphasizes the importance of a multidisciplinary team approach at high-volume centers for optimal outcomes.
Colorectal liver metastases multidisciplinary approach 2 (2)
This document discusses treatment options for colorectal liver metastases. It summarizes that resection provides the best chance for long-term survival, with 5-year survival rates of 45-60%. Radiofrequency ablation can treat small, unresectable tumors but does not replace resection. For resectable tumors, options include chemotherapy with or without resection. A multidisciplinary team approach is important for evaluating all treatment possibilities.
Ovary 1
This document discusses the management of ovarian cancer. It covers risk-reducing salpingo-oophorectomy (RRSO) for high-risk patients, surgical staging techniques including open and minimally invasive approaches, management of early-stage disease including adjuvant chemotherapy and radiation, cytoreductive surgery and goals for advanced-stage disease, and the role of interval debulking surgery after neoadjuvant chemotherapy. Complete resection of all tumor is the optimal outcome for advanced ovarian cancer to improve survival outcomes.
management of Liver cancers
This document outlines recent advances in the management of liver cancers. It discusses the epidemiology, risk factors, classification, investigations and various treatment options for liver cancers including hepatic resection, ablation techniques, regional therapies, chemotherapy and transplantation. Resection remains the standard curative treatment for non-cirrhotic patients with localized disease, while ablation techniques and regional therapies are alternatives for patients not eligible for surgery. Advances in surgical techniques and anesthesia have improved resection outcomes.
Carcinoma stomach management
Carcinoma of the stomach is usually suspected based on symptoms like abdominal pain or indigestion. Investigations include endoscopy with biopsy, which is the gold standard for diagnosis. Staging involves endoscopic ultrasound, CT, PET scans and laparoscopy. Treatment depends on the stage, and may involve surgery such as gastrectomy with lymph node dissection, adjuvant chemotherapy and/or radiotherapy. Prognosis depends on factors like stage, lymph node involvement and response to treatment, with 5-year survival rates ranging from 95% for early stage to near 0% for metastatic disease.
Hepatocellular carcinoma 2020
This document provides an overview of the management of hepatocellular carcinoma (HCC). It discusses the epidemiology, risk factors, diagnosis and staging, as well as treatment options for HCC. The major risk factors for HCC include hepatitis B virus, hepatitis C virus, and alcohol. Treatment depends on the stage and includes options such as liver transplantation, resection, ablation, transarterial chemoembolization, and the systemic therapy sorafenib. Prevention through vaccination and treating underlying liver diseases can help reduce cases of HCC.
Rectal cancer alex
1. Rectal cancer is a common malignancy that arises in the rectum, usually within 15 cm of the anal verge.
2. Diagnostic workup includes physical exam, proctoscopy, biopsy of the primary tumor, and imaging. Blood tests like CEA are also done.
3. Treatment involves a multidisciplinary approach with surgery, often total mesorectal excision, along with pre- or post-operative chemoradiation to reduce the risk of recurrence. The type of surgery depends on how far the cancer has spread.
Carcinoma esophagus
This document provides an overview of carcinoma of the esophagus, including epidemiology, etiology, classification, diagnosis, staging, and management. It discusses the different types of esophageal cancer, risk factors, pre-malignant conditions, patterns of spread, diagnostic tools such as endoscopy and imaging, and the AJCC staging system. Treatment options are covered for early stage disease including endoscopic resection and ablation methods, as well as surgical approaches for localized and advanced disease, including transhiatal esophagectomy, Ivor-Lewis esophagectomy, and McKeown esophagectomy. Post-operative complications are also reviewed.
gastriccancer
This document discusses gastric cancer, including its epidemiology, risk factors, diagnosis, treatment, and outcomes. Some key points:
- Gastric cancer is the 4th most common cancer worldwide and the 15th most common in the US. Incidence has declined significantly over the last century.
- Risk factors include H. pylori infection, smoking, diet high in salted/smoked foods, and adenomatous polyps.
- Diagnosis is typically made via endoscopy with biopsy. Staging may involve endoscopic ultrasound, CT scan, or laparoscopy.
- Treatment is usually surgical resection with D1 or D2 lymph node dissection and chemotherapy/radiation. Total or
Rathod Gastric Cancer Presentation final.pptx
- Gastric cancer is the fourth most common cancer worldwide and the second leading cause of cancer death. It is more common in older individuals, males, and those in East Asia. Risk factors include H. pylori infection, dietary factors like salt and smoking, and hereditary conditions.
- Staging workup includes endoscopy with biopsy, EUS, CT, PET, and laparoscopy to determine depth of invasion, lymph node involvement, and metastasis. Surgery is the main treatment and may be combined with chemotherapy or radiation depending on stage. Outcomes have improved with more extensive lymph node dissection and adjuvant therapy. Palliative options exist for advanced or unresectable cases.
Rectal Carcinoma
This document provides an overview of rectal carcinoma. It discusses the epidemiology, risk factors, clinical presentation, investigations, staging, and treatment options. Rectal carcinoma is the third most common cause of cancer deaths in the USA, with over 150,000 new cases diagnosed annually. Treatment may involve local excision, low anterior resection, abdominoperineal resection, or multivisceral resection depending on the stage, size, and location of the tumor. Total mesorectal excision and adjuvant chemoradiation are important to reduce local recurrence rates.
Hcc
1) Surgical management of hepatocellular carcinoma (HCC) in Egypt must be seen in the context of various treatment modalities like resection, transplantation, and interventional radiology which should be used in a complementary rather than exclusive manner.
2) Liver transplantation according to the Milan criteria provides the best oncologic outcomes for HCC but has limitations related to tumor size and number as well as donor availability. Surgical resection remains important for patients outside transplant criteria.
3) Surgical techniques have improved outcomes with resection, including careful patient selection, mapping of lesions, and attention to surgical details to achieve low mortality and recurrence rates. Bridging therapies and downstaging can increase transplant eligibility.
Role of surgery in metastatic colorectal cancer
Surgery plays an important role in treating metastatic colorectal cancer. The document discusses:
1) The liver is the most common site of metastasis and surgical resection of isolated liver metastases can provide a 5-year survival rate of 45-60%, compared to just 6-9 months with no treatment.
2) Other potentially resectable isolated metastases, such as those in the lungs or peritoneum, may also be treated with surgery, providing 5-year survival rates around 20-40%.
3) Neoadjuvant chemotherapy can downsize initially unresectable liver metastases to make them resectable and improve long-term outcomes compared to surgery alone.
pancreatic cas managementby bedrumoh.pptx
1. Pancreatic cancer is the 4th leading cause of cancer death and often presents with jaundice, abdominal pain, weight loss, or new-onset diabetes. Diagnosis involves blood tests, CT, MRI, EUS, and biopsy.
2. Surgical management includes Whipple procedure for head tumors or distal pancreatectomy for body/tail tumors. Palliative options relieve biliary/duodenal obstruction and pain via stenting, bypass, or celiac plexus block.
3. Adjuvant chemo-radiotherapy after surgery can increase survival compared to surgery alone. Neoadjuvant FOLFIRINOX increases resectability of borderline resect
Management of Carcinoma Rectum.pptx
- Management of rectal cancer has changed dramatically in recent decades with multimodality treatment becoming standard.
- Surgery remains the primary treatment but local recurrence rates were historically high at 20-50% with surgery alone.
- Total mesorectal excision has significantly reduced local recurrence rates by completely removing the mesorectum containing the tumor and draining lymph nodes.
- Adjuvant chemoradiation or neoadjuvant chemoradiation further lower recurrence rates and improve survival compared to surgery alone.
Similar to ca colorectal powerpoint explanation inn (20)
Colorectal liver metastases multidisciplinary approach 2 (2)
Colorectal liver metastases multidisciplinary approach 2 (2)
Colorectal liver metastases multidisciplinary approach 2 (2)
Colorectal liver metastases multidisciplinary approach 2 (2)
Recently uploaded
Identification and nursing management of congenital malformations .pptx
Identification and nursing management of congenital malformations .pptxMGM SCHOOL/COLLEGE OF NURSING
Identification and nursing management of congenital malformations ABDOMINAL TRAUMA in pediatrics part one.
Abdominal trauma in pediatrics refers to injuries or damage to the abdominal organs in children. It can occur due to various causes such as falls, motor vehicle accidents, sports-related injuries, and physical abuse. Children are more vulnerable to abdominal trauma due to their unique anatomical and physiological characteristics. Signs and symptoms include abdominal pain, tenderness, distension, vomiting, and signs of shock. Diagnosis involves physical examination, imaging studies, and laboratory tests. Management depends on the severity and may involve conservative treatment or surgical intervention. Prevention is crucial in reducing the incidence of abdominal trauma in children.
Promoting Wellbeing - Applied Social Psychology - Psychology SuperNotes
A proprietary approach developed by bringing together the best of learning theories from Psychology, design principles from the world of visualization, and pedagogical methods from over a decade of training experience, that enables you to: Learn better, faster!
share - Lions, tigers, AI and health misinformation, oh my!.pptx
• Pitfalls and pivots needed to use AI effectively in public health
• Evidence-based strategies to address health misinformation effectively
• Building trust with communities online and offline
• Equipping health professionals to address questions, concerns and health misinformation
• Assessing risk and mitigating harm from adverse health narratives in communities, health workforce and health system
The Electrocardiogram - Physiologic Principles
These lecture slides, by Dr Sidra Arshad, offer a quick overview of the physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar lead (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
6. Describe the flow of current around the heart during the cardiac cycle
7. Discuss the placement and polarity of the leads of electrocardiograph
8. Describe the normal electrocardiograms recorded from the limb leads and explain the physiological basis of the different records that are obtained
9. Define mean electrical vector (axis) of the heart and give the normal range
10. Define the mean QRS vector
11. Describe the axes of leads (hexagonal reference system)
12. Comprehend the vectorial analysis of the normal ECG
13. Determine the mean electrical axis of the ventricular QRS and appreciate the mean axis deviation
14. Explain the concepts of current of injury, J point, and their significance
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. Chapter 3, Cardiology Explained, https://www.ncbi.nlm.nih.gov/books/NBK2214/
7. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
#cALL# #gIRLS# In Dehradun ꧁❤8107221448❤꧂#cALL# #gIRLS# Service In Dehradun W...
#cALL# #gIRLS# In Dehradun ꧁❤8107221448❤꧂#cALL# #gIRLS# Service In Dehradun W...chandankumarsmartiso
#cALL# #gIRLS# In Dehradun ꧁❤8107221448❤꧂#cALL# #gIRLS# Service In Dehradun Women Seeking Service
TEST BANK For Community Health Nursing A Canadian Perspective, 5th Edition by...
TEST BANK For Community Health Nursing A Canadian Perspective, 5th Edition by Stamler, Verified Chapters 1 - 33, Complete Newest Version Community Health Nursing A Canadian Perspective, 5th Edition by Stamler, Verified Chapters 1 - 33, Complete Newest Version Community Health Nursing A Canadian Perspective, 5th Edition by Stamler Community Health Nursing A Canadian Perspective, 5th Edition TEST BANK by Stamler Test Bank For Community Health Nursing A Canadian Perspective, 5th Edition Pdf Chapters Download Test Bank For Community Health Nursing A Canadian Perspective, 5th Edition Pdf Download Stuvia Test Bank For Community Health Nursing A Canadian Perspective, 5th Edition Study Guide Test Bank For Community Health Nursing A Canadian Perspective, 5th Edition Ebook Download Stuvia Test Bank For Community Health Nursing A Canadian Perspective, 5th Edition Questions and Answers Quizlet Test Bank For Community Health Nursing A Canadian Perspective, 5th Edition Studocu Test Bank For Community Health Nursing A Canadian Perspective, 5th Edition Quizlet Test Bank For Community Health Nursing A Canadian Perspective, 5th Edition Stuvia Community Health Nursing A Canadian Perspective, 5th Edition Pdf Chapters Download Community Health Nursing A Canadian Perspective, 5th Edition Pdf Download Course Hero Community Health Nursing A Canadian Perspective, 5th Edition Answers Quizlet Community Health Nursing A Canadian Perspective, 5th Edition Ebook Download Course hero Community Health Nursing A Canadian Perspective, 5th Edition Questions and Answers Community Health Nursing A Canadian Perspective, 5th Edition Studocu Community Health Nursing A Canadian Perspective, 5th Edition Quizlet Community Health Nursing A Canadian Perspective, 5th Edition Stuvia Community Health Nursing A Canadian Perspective, 5th Edition Test Bank Pdf Chapters Download Community Health Nursing A Canadian Perspective, 5th Edition Test Bank Pdf Download Stuvia Community Health Nursing A Canadian Perspective, 5th Edition Test Bank Study Guide Questions and Answers Community Health Nursing A Canadian Perspective, 5th Edition Test Bank Ebook Download Stuvia Community Health Nursing A Canadian Perspective, 5th Edition Test Bank Questions Quizlet Community Health Nursing A Canadian Perspective, 5th Edition Test Bank Studocu Community Health Nursing A Canadian Perspective, 5th Edition Test Bank Quizlet Community Health Nursing A Canadian Perspective, 5th Edition Test Bank Stuvia
A Classical Text Review on Basavarajeeyam
Basavarajeeyam is a Sreshta Sangraha grantha (Compiled book ), written by Neelkanta kotturu Basavaraja Virachita. It contains 25 Prakaranas, First 24 Chapters related to Rogas& 25th to Rasadravyas.
NVBDCP.pptx Nation vector borne disease control program
NVBDCP was launched in 2003-2004 . Vector-Borne Disease: Disease that results from an infection transmitted to humans and other animals by blood-feeding arthropods, such as mosquitoes, ticks, and fleas. Examples of vector-borne diseases include Dengue fever, West Nile Virus, Lyme disease, and malaria.
Osteoporosis - Definition , Evaluation and Management .pdf
Osteoporosis is an increasing cause of morbidity among the elderly.
In this document , a brief outline of osteoporosis is given , including the risk factors of osteoporosis fractures , the indications for testing bone mineral density and the management of osteoporosis
How STIs Influence the Development of Pelvic Inflammatory Disease.pptx
STIs may cause PID. For the both disease, herbal medicine Fuyan Pill can be a solution.
Histololgy of Female Reproductive System.pptx
Dive into an in-depth exploration of the histological structure of female reproductive system with this comprehensive lecture. Presented by Dr. Ayesha Irfan, Assistant Professor of Anatomy, this presentation covers the Gross anatomy and functional histology of the female reproductive organs. Ideal for students, educators, and anyone interested in medical science, this lecture provides clear explanations, detailed diagrams, and valuable insights into female reproductive system. Enhance your knowledge and understanding of this essential aspect of human biology.
Recently uploaded (20)
Identification and nursing management of congenital malformations .pptx
Identification and nursing management of congenital malformations .pptx
Promoting Wellbeing - Applied Social Psychology - Psychology SuperNotes
Promoting Wellbeing - Applied Social Psychology - Psychology SuperNotes
share - Lions, tigers, AI and health misinformation, oh my!.pptx
share - Lions, tigers, AI and health misinformation, oh my!.pptx
#cALL# #gIRLS# In Dehradun ꧁❤8107221448❤꧂#cALL# #gIRLS# Service In Dehradun W...
#cALL# #gIRLS# In Dehradun ꧁❤8107221448❤꧂#cALL# #gIRLS# Service In Dehradun W...
TEST BANK For Community Health Nursing A Canadian Perspective, 5th Edition by...
TEST BANK For Community Health Nursing A Canadian Perspective, 5th Edition by...
NVBDCP.pptx Nation vector borne disease control program
NVBDCP.pptx Nation vector borne disease control program
Osteoporosis - Definition , Evaluation and Management .pdf
Osteoporosis - Definition , Evaluation and Management .pdf
CHEMOTHERAPY_RDP_CHAPTER 6_Anti Malarial Drugs.pdf
CHEMOTHERAPY_RDP_CHAPTER 6_Anti Malarial Drugs.pdf
How STIs Influence the Development of Pelvic Inflammatory Disease.pptx
How STIs Influence the Development of Pelvic Inflammatory Disease.pptx
Vestibulocochlear Nerve by Dr. Rabia Inam Gandapore.pptx
Vestibulocochlear Nerve by Dr. Rabia Inam Gandapore.pptx
ca colorectal powerpoint explanation inn
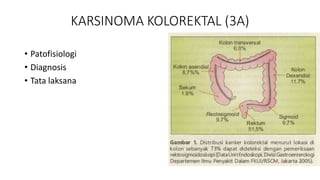
- 1. KARSINOMA KOLOREKTAL (3A) • Patofisiologi • Diagnosis • Tata laksana
- 3. DIAGNOSIS • Klinis • LAB • Anemia def Fe • FOBT
- 4. STAGING
- 5. We recommend that average-risk patients over the age 45 years be screened for CRC.
- 6. TATA LAKSANA
- 7. LOKAL • Approximately 80 percent of cancers are localized to the colon wall and/or regional nodes. • Surgery is the only curative modality for localized colon cancer. • The goal complete removal of the tumor, the major vascular pedicle, and the lymphatic drainage basin of the affected colonic segment. • Restoration of bowel continuity using a primary anastomosis • Temporary proximal diverting colostomy or ileostomy
- 10. Metastatic • 20 to 25 percent of newly diagnosed colon cancers • The most common distant metastatic sites : liver, lungs, lymph nodes, and peritoneum. • Systemic chemotherapy improved median survival from less than one year to more than 30 months, • fewer than 20 % of those treated with chemotherapy still alive at five years.