Downloaded 15 times

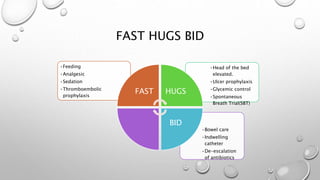
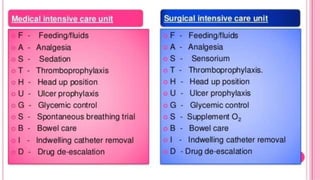

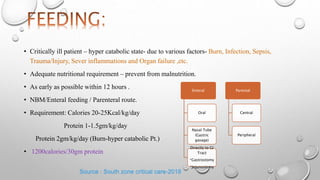


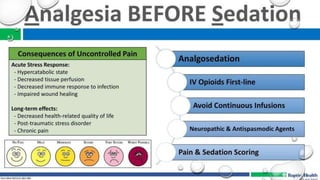




This document discusses various care bundles for critically ill patients, including: - Nutrition bundles to provide adequate calories and protein within 12 hours to prevent malnutrition. - Pain management bundles using pharmacological and non-pharmacological approaches. - Ventilator bundles like daily sedation holds to assess readiness for extubation. - Thromboprophylaxis bundles using mechanical methods like foot pumps and pharmacological methods like low molecular weight heparin.















































