An expert inbreaking bad news is not someone who gets it right every
time – he or she is merely someone who gets it wrong often.
- Buckman
3.
Introduction
• Breaking badnews is an important part of the health care
professional's job and requires experience and expertise.
• Breaking bad news is a skill that can be learned and can be used in a
busy clinical practice
4.
BAD NEWS
• Anynews that drastically and negatively alters the patients views of
his/her future. Buckman 1992
• when an illness is life-threatening, there exists the potential for many
emotionally charged and potentially conflict-creating moments
collectively called “bad news” situations
• In these situations empathic and effective communication skills are
essential.
• The "badness" of bad news is the gap between the patient's
expectations and the medical reality.
5.
Examples of badnews
• Death
• Chronic diseases e.g. Diabetes, Hypertension
• Terminal diseases e.g. cancer
• Infectious diseases like HIV, Hepatitis
• Poor prognosis related to chronic diseases e.g. heart failure, CVA
• Intra uterine foetal death
• Disease recurrence
• Debilitating diseases like Alzheimer’s disease, Multiple sclerosis
8.
WHY SHOULD ITBE DONE
Improve the patient’s and family’s ability to plan and cope
Encourage realistic goals and autonomy
Support the patient emotionally
Strengthen patient-doctor relationship
Foster collaborating among the patient, family, doctor and
professionals
Reduces stress in doctors
Avoid conflicts between patients family and doctors
9.
Common barriers tobreaking bad news
1. The doctor is not sure about what the patient is expecting
2. The doctor fears that he may be destroying the hope of the patient.
3. The doctor may fear that he himself may not be adequately capable
of dealing with an uncontrollable disease.
4. The doctor may fear that he is incapable of managing the emotional
reactions resulting from breaking the news
5. The doctor might have presented an overoptimistic picture of the
patient’s condition in the past and this may be causing embarrassment
in the current situation where he needs to break the bad news
10.
BREAKING BAD
NEWS
DO’S
• Allowfor silence as well as emotional
reactions.
• Give time Be sensitive to the
nonverbal language.
• Document and liaise with the
multidisciplinary team.
• Use simple language and honest
communication.
• Ensure privacy and confidentiality.
• Listen to what the patient says
DON’T’S
• Assuming that you know what
concerns the patient.
• Make judgmental comments.
• Distort the truth.
• Keep talking all the time.
• Give false reassurance.
• Overload with information.
• Withhold information
11.
APPROACHES TO COMMUNICATINGBAD NEWS
• Physicians and health care providers caring for patients with
significant or advanced illnesses should develop a standardized
approach for sharing important information and planning
interventions.
• Any approach has 2 components
Divulging of information: by which you impart information to the
patient
Therapeutic dialogue: by which you listen to, hear, and respond to
the patient's reactions to the information
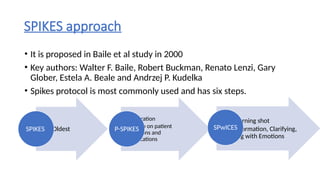
SPIKES approach
• Itis proposed in Baile et al study in 2000
• Key authors: Walter F. Baile, Robert Buckman, Renato Lenzi, Gary
Glober, Estela A. Beale and Andrzej P. Kudelka
• Spikes protocol is most commonly used and has six steps.
Oldest
SPIKES
• Preparation
• No step on patient
questions and
clarifications
P-SPIKES
• W- Warning shot
• ICE-Information, Clarifying,
dealing with Emotions
SPwICES
16.
P-SPIKES
(1) Prepare forthe discussion
(2) Set up a suitable environment
(3) Begin the discussion by finding out what the patient and/or family
understand
(4) Determine how they will comprehend new information best and how
much they want to know
(5) Provide needed new knowledge accordingly
(6) Allow for emotional responses
(7) Share plans for the next steps in care
17.
• Mentally preparefor the interaction with
the patient or family.
• Review what information needs to be
communicated.
• Plan how you will provide emotional
support.
• Rehearse key steps and phrases in the
interaction.
18.
Ensure the appropriatesetting
for a serious and potentially
emotionally charged
discussion.
Ensure that patient, family
and appropriate social
supports are present.
Devote sufficient time.
Ensure privacy and prevent
interruption by people and
beepers.
Bring a box of tissues.
19.
P-PATIENTS PERCEPTIONAND
PREPARATION
• Begin the discussion by establishing the baseline and whether the
patient and family can grasp the information.
• Start with open ended questions to encourage participation.
-what do you understand about your illness?
-when you first had symptom x,what do you think it might be?
-what did Dr.x tell you when he or she sent you here?
-what do you think is going to happen?
20.
I-INVITATION ANDINFORMATION NEEDS
• Discover what information needs the patient and/or family have and
what limits they want regarding the bad information.
• Possible questions to use:
• If this condition turns out to be something serious, do you want to
know?
• Would you like me to tell you all the details of your condition? If not,
who would you like me to talk to?
21.
• Provide thebad news or
other information to the
patient and/or family
sensitively.
• Do not just dump the
information on the patient
and family.
• Check for patient and family
understanding.
22.
EMPATHY AND EXPLORATION
•Identify the cause of the emotions— e.g.,
poor prognosis.
• Empathize with the patient’s and/or family’s
feelings.
• Explore by asking open-ended questions
• Strong feelings in reaction to bad news are
normal.
• Acknowledge what the patient and family are
feeling.
• Remind them such feelings are normal, even
if frightening.
• Give them time to respond.
• Remind the patient and family you won’t
abandon them.
23.
• Delineate forthe patient
and the family the next
steps, including additional
tests or interventions.
• It is the unknown and
uncertain that can increase
anxiety.
• Recommend a schedule
with goals and landmarks.
• Provide your rationale for
the patient and/or family to
accept (or reject).
• If the patient and/or family
are not ready to discuss the
next steps, schedule a
follow-up visit.
PEWTER MODEL
• P:Preparing the one giving the news through education and training,
and preparing the setting and the approach for giving the news.
• E: Evaluating what the listener already knows.
• W: Warning by making a brief statement followed by a moment of
silence to prepare the listener for the bad news that comes next.
• T: Telling the news.
• E: Emotional response: paying attention to and responding
appropriately to the listener’s emotional responses.
• R: Regrouping by helping the listener move forward with the next
steps.
DOCUMENTATION
• Documentation isvery essential in breaking bad news.
• Accurate records of conversations should be maintained in the
patient’s file.
• Key elements to document include:
• The diagnosis
• Management options discussed
• Exact words and expressions used while delivering the news
• Proper documentation aids communication with the care team and
ensures effective follow-up.
29.
RESPONSES TO RECEIVINGBAD NEWS
• Reactions to bad news vary greatly.
• Perception of "bad news" is individual and subjective.
• Our Focus :
• Is not on labeling reactions as normal or abnormal.
• Is the reaction helping the patient to cope?
• If not, identify ways to reduce the patient’s distress.
30.
RESPONSES TO RECEIVINGBAD NEWS
Criteria for assessing and responding to patient reaction include:
• Social acceptability: A reaction has to be within the bounds of cultural norms and
rules
• Adaptability: does the reaction increase or decrease the patient's distress at his
or her situation?
• Fixability: if the reaction is increasing the patient's distress, are there any
interventions that might help?
MAIN REACTIONS TOBAD NEWS
Adaptive
• Some reactions may appear to the
abnormal to you, but are not abnormal
for that patient and may be helping the
patient to recover.
Maladaptive
• Reaction may appear to be socially or
culturally desirable but may actually
prevent a patient from truly coping with
the news
33.
References
• Harrison’s principlesof internal medicine 21st
edition
• Hazzard’s Geriatric medicine and Gerontology
• How to Break Bad News - A Guide for Health Care Professionals

















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








