2. Clinical disease: Presentation of both the types is same.
- Onset: abrupt
- High fever, shaking shills, delirium, severe muscle ache, bone and joint pain
- Neurological complications: Lymphocytic meningitis
Facial palsy
- During relapse, each cycle –less severe than preceding one
- A rash may develop during initial attack
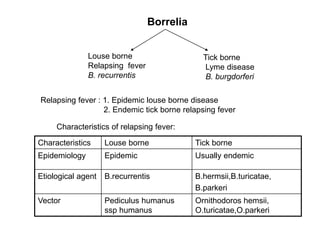
Characteristics Louse borne Tick borne
Primary attack 5.5 days 3 days
Asymptomatic interval 9 days 7 days
Number of relapse 3 1
Duration of relapse 2 days 2.5 days
3. Laboratory diagnosis
• Isolation is difficult
• Mainstay of diagnosis– demonstration of Borrelia in PBS
Sample collected: Blood—during the height of fever
• Smears: 1. Dark field microscopy
2. Thin and thick smears: stained by Giemsa/ Leishman
• Culture: Difficult and less sensitive
• Serology: Not useful. VDRL comes positive in 5-10% cases
Giemsa-Wright stain on PBS
4. Lyme disease
In 1977: children developed unusual type of arthritis in Lyme, USA
In 1982: Offending bacteria: B.burgdorferi, was isolated by Burgdoofer
Reservoirs: Deer,mice,rodents
Transmission to man: by the bite of tick— Ixodes ricinus and Ixodes dammini
Clinical Syndrome
1. Early stage: Characterized by Erythema migrans
Lesion at the site of tick bite
small macule/papule
Annular with necrotic center, raised , red border (bull’s-eye)
Early symptoms: malaise, severe fatigue, headache, fever, mascular pain
5.
6. 2. Late stage: In 80% untrated cases
Two phases----
• Neurologic and cardiological--
Meningitis, encephalitis, pheripheral nerve neuropathy
Cardiac dysfunction: heart block, myopericarditis,
congestive heart failure
• Arthritis,arthralgia
Laboratory diagnosis
Organism: rarely seen in specimen
Diagnosis: clinical
Erythema mograns: diagnostic
Staining: Blood, CSF sediment : DFM
Giemsa, Wright stained PBS
Culture: Blood, CSF, Edge of the lesion---Rare
Serology: Not much useful
Immunoflurescence, ELISA
8. Vincent’s angina
• Etiologic agent: B.vincenti
• Commensal of oropharynx
• Cultured in media: ascitic fluid,serum
• Grows well in mixed cultures with Fusobacterium
• Disease: Vincent’s angina: Ulcerative oropharyngitis With anerobic
Gingivostomatitis fusiform bacilli
• Sample: exudate from the lesion
• Cultivation: difficult, done anaerobically
9. Leptospiraceae
1886: Adolf Weil: described spirochaetal jaundice
1907: Named as Spirochaeta interrogans
Shape resembling interrogation (question) mark
1915: Inada: named it as Leptospira icterohaemorrhagae
10. LEPTOSPIROSIS
• Re-emerging infectious disease
• Zoonotic disease .
• Occupational disease: Farmers,
sewer workers,veterinarians,etc.
• Recreational disease : Swimmers,
water rafters, hunters
• It is endemic in India & has
epidemic potential
11. Order : Spirochaetales
Family : Leptospiraceae
Genus : Leptospira
Species : interrogans - pathogenic strains
biflexa - saprophytic strains
• Spiral bacteria
• Tightly coiled, 6-12 m in length & 0.1 m
in diameter
• Each cell-18 or more coils
• Helical amplitude 0.1 to 0.15 m
• Wavelength approx.0.5 m
• Pointed ends, bent into a distinctive hook
LEPTOSPIROSIS - The culprit: Leptospira
12. MODE OF TRANSMISSION
• Direct exposure to the infected animals
• Exposure to an environment contaminated with urine,
blood, tissues of infected animal
• Entry
– Inflamed/Broken skin
– Intact mucous membrane
– Conjunctiva
• Water-borne infection -documented
• Infection through inhalation –documented
• Human to human transmission-very rare
13. Clinical presentations of
Leptospirosis
Greatest mimicker of disease !
• Icteric manifestations:
- jaundice develops about 3rd to 7th day
- Weil’s disease - when associated
with renal dysfunction
• Anicteric manifestations
16. Dark Field Microscopy
• Least sensitive and specific
• Requires 10,000-20,000 organisms/ml
• Fibrin strands and erythrocyte
membranes can be confused with
leptospires.
• Not recommended for diagnosis
• Only for culture confirmation
• Urine : alkalized
20. Cultivation of Leptospires
• Difficult to grow,Requires albumin, serum
• Grow at 300C
• Takes approximately 3 weeks to grow
• Media containing rabbit serum: Fletcher,
Korthoff, Noguchi,
• Most widely used medium based on the
oleic acid-albumin medium is EMJH
22. Serology
Detection of antibodies to Leptospires
1. Genus specific tests
2. Serogroup/serovar specific tests
Microscopic Agglutination Test (MAT)
WHO Reference Standard
Older
MSAT
IFAT
IHA
Newer
ELISA
Lepto-Dipstick
Lepto dri-dot
Lepto lateral flow
23. Specimen for serology
• 5 ml of venous blood in a plain test tube
• Paired serum samples
• Time of collection
1st sample – as soon as possible & prior to
antibiotic therapy
2nd sample – after an interval of at least 7
days
• Four fold rise in antibody titers must be
demonstrated
28. Microscopic Agglutination Test
(MAT)
Gold standard
Serovar/serogroup specific
Reference laboratory
A large panel of serovars (live
organisms) used as antigens.
Technically difficult.
Positive titre >/= 1:200 for single
samples
30. LEPTOSPIROSIS OUTBREAKS
PLACE YEAR SOURCE
MUMBAI 1983 RAT INFESTED
POND
MUMBAI 1999, 2000,
2001
? DRAIN WATER
KANKAVALI 1998,1999,
2000
RICE FIELD
NAGPUR 1998,1999 SEWAGE
FARMING
GUJARAT 1997, 2000 UNKNOWN
31. Prophylaxis & Therapy
Rodent control measures & hygiene
Protective clothing for high risk
occupations
Vaccination of animals
Therapy: Penicillin G
Doxycycline
Ampicillin