Bone is aspecialized form of mineralized
connective tissue . Skeletal system is vital to life as
it provides mechanical support and mineral
homeostasis .
Diseases associated with decreased bone mass
Osteoporosis is a disease characterized by
increased porosity of skeleton resulting from
reduced bone mass. The bones are prone
fracture.
Osteoporosis
3.
Osteoporosis may bedue to disuse or
metabolic bone disease. Most common forms
of osteoporosis are senile and post menopausal
osteoporosis.
Persistant failure of mineralization in adults
leads to eventual loss of skeletal mass referred
to as osteopenia . Osteoporosis is a type of
osteopenia.
Osteopenia
4.
Pyogenic osteomyelitis
Organisms mayreach the bone by 1)
haematogenous spread 2) extension from
Infections –Osteomyelitis
Osteomyelitis denotes inflammation of bone
and marrow (myelo- marrow) . All types of
organism can cause osteomyelitis. But
infections caused by certain pyogenic bacteria
and mycobacterium tuberculosis are the most
common
5.
contiguous site 3)direct implantation
Most cases of osteomyelitis are
hematogenous in origin and develop in long
bones or vertebral bodies . Staphylococcus is
the causative organism in 80-90 % of cases .
Morphology: Depending upon the duration
Osteomyelitis may be acute, subacute or
chronic. Infection begins in the metaphyseal
end . Bacteria proliferate , induce an acute
inflammatory reaction and cause cell death .
6.
Entrapped bone undergoesnecrosis . The
bacteria and inflammation spread within the
shaft of the bone and reach the periosteum .
There it forms sub periosteal abscess .It may
penetrate through the cortex forming
draining skin sinus tract . In children
periosteum is lifted off,since it is loosely
attached . This further impairs the blood
supply of the affected region causing
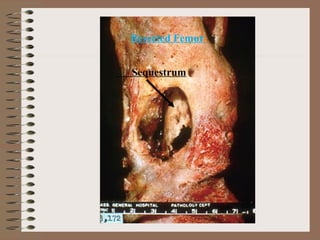
segmental bone necrosis. Dead piece of bone
is known as sequestrum
7.
With passage oftime there is formation of new
bone beneath the periosteum . This forms an
encasing sheath around the necrosed bone and
is known as involucrum . Involucrum has
irregular surface and has perforation through
which the discharging sinus tracts pass .
Long continued new bone formation gives
rise to dense sclerotic pattern of
osteomyelitis called chronic sclerosing
osteomyelitis of Garre’
Occasionally acute osteomyelitismay be
contained to a localised area and walled off by
fibrous tissue and granulation tissue . This
termed Brodie’s abscess .
Complications
1) pathologic fracture 2) secondary
amyloidosis 3) endocardits 4) sepsis 5)
Development of squamous cell carcinoma in
the sinus tract ( epithelialized) 6) rarely
sarcoma in infected bone
10.
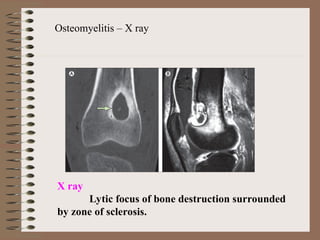
Osteomyelitis – Xray
X ray
Lytic focus of bone destruction surrounded
by zone of sclerosis.
11.
Pagets Disease (Osteitis Deformans)
Paget disease is divided into 1) an initial
osteolytic stage followed by 2) a mixed
osteoclastic – osteoblastic stage which ends with
a predominance of obsteoblastic activity and
evolves ultimately into 3) a burnt out quiescent
osteosclerotic stage . Thus there is a repetitive
and overlapping sequence . The net effect of
this process is a gain in bone mass . However
the newly formed bone is disordered and
architecturally unsound
12.
Usually begin inmid adulthood.
Bones are vulnerable to deformation under
stress . Chalk stick fractures are a common
complication . A variety of tumors can arise in
paget disease . There include giant cell tumor
and osteosarcoma
Pathogenesis : Believed to be due to both
environmental and genetic factors. Gene
mutations trigger inflammatory factors .
Current evidence suggests an infection by
Measles and, other RNA viruses can also
cause this .
Histology: shows mosaic pattern of lamellar
bone .
Most common skeletalmalignancy is
metastasis . Osteosarcoma is the most
common primary tumour of bone .
Malignant
Ewing tumour
Adamantinoma
Metastatic tumours
16.
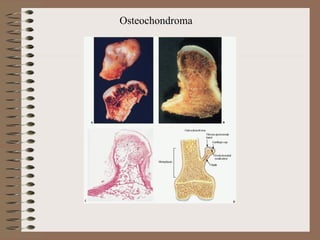
Osteochondroma
Also known asexostosis . This is a benign
cartilage capped outgrowth that is attached to
the underlying skeleton by a bony stalk .
Occurs in late adolescence and early adulthood
Arise from metaphysis near the growth plate
of long tubular bone especially about the knee
Morphology : Osteochondromas are
mushroom shaped . Cap is composed of hyaline
cartilage. Bone forms the inner portion of head
and stalk. Cortex of the stalk merges with the
cortex of the host bone with continuity of
medullary cavity. The continuity of marrow
cavity of both host and tumour bone is a
characteristic finding on x-ray
Giant cell tumourGiant cell tumour is so
named because it contains numerous
multinucleated osteoclast like giant cells. Hence
the name osteoclastoma . It is a benign but
locally aggressive neoplasm . Occurs in twenties
to forties .
Pathogenesis: In normal bone osteoblasts lay
down new bone . They arise from primitive
mesenchymal cells. Osteoclasts eat up aged
bone . They arise from haempoietic progenitor
cells (which also give rise to monocyte
macrophage lineage.) Neoplastic cells of GCT
are mononuclear cells which are osteoblast
precursors . They express
19.
Gross : Tumoursare large and red brown and
undergo cystic degeneration
high RANKL which activate bone osteoclasts
causing destructive resorption of bone seen
grossly as cystic change. Multinucleate giant
cells seen in GCT are reactive and are
multinucleate osteoclast type .
22.
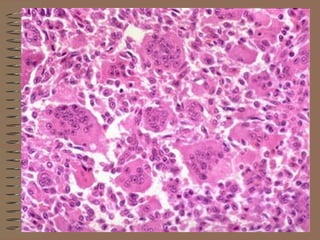
Microscopy : Uniformoval mononuclear
cells growing in a syncytium . Mononuclear
cells are the proliferating component of the
tumour and mitoses are frequent .
Scattered within the background are
numerous osteoclast type giant cells having
100 or more nuclei similar to that of
mononuclear cells . Necrosis,hemorrhage,
hemosiderin deposition and reactive bone
formation are common secondary features
24.
Giant cell tumoursin adults involve both
epiphysis and metaphysis . But in adolescents
They are confined to metaphysis. Commonest
location of the tumour is around the knee
(distal femur and proximal tibia )
X- ray Large purely lytic eccentric lesion
eroding into subchondral bone plate .
Overlying cortex is destroyed producing a
bulging soft tissue mass delineated by a thin
shell of reactive bone Margins with adjacent
bone is circumscribed but seldom sclerotic .
25.
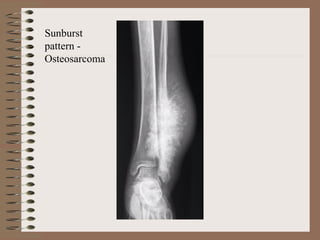
Osteosarcoma
Osteosarcoma is definedas a malignant
mesenchymal tumour in which the cancerous
cells produce bone matrix . It has a bimodal
age distribution 75% occurs in patients
younger than age 20 . There is a smaller peak
in elderly in whom secondary osteosarcoma
occurs
-arise from metaphyseal region of long bones
of the extremities usually about the knee joint
26.
Pathogenesis : mutationsare fundamental to
the development of osteosarcoma . Notable
mutations being those of RB gene, TP53.
CDKN2A, MDM2 , CDK4
Morphology: Several subtypes of
osteosarcomas are recognized and are
grouped according to
- anatomic portion of bone from
which they arise
(Intramedullary ,
Intracortical ,Surface )
27.
- Degree ofdifferentiation
-Multicentricity ( synchronous,
metachronous) -Primary or
secondary to other bone
disorders such as paget disease ,
benign tumours , bone infarcts ,
previous irradiation rarely
osteomyelitis -Histologic
variants( osteoblastic ,
chondroblastic , fibroblastic , small
cell & giant cell)
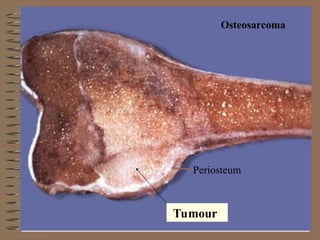
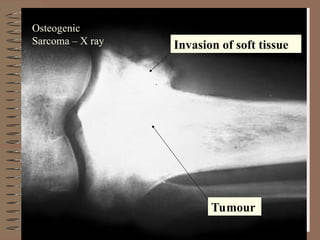
Gross : Osteosarcomas are bulky tumours that
are gritty , gray- white and often contain areas
28.
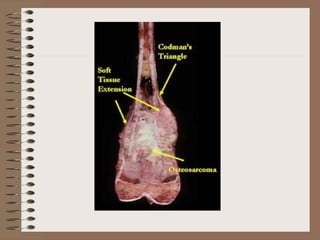
of haemorrhage andcystic degeneration.
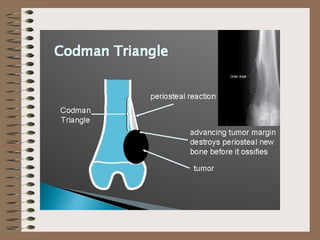
Codman‘s triangle formed by the tumour
lifting the periosteum and forming a triangle
between the periosteum and the bone is seen.
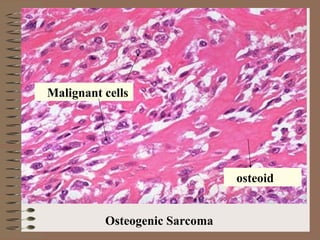
Microscopy : The hallmark of osteosarcoma is
the formation of osteoid by malignant
mescenchymal cells. This is seen in the form of
islands of primitive bony trabeculae ( osteoid)
hugged by a rim of malignant osteoblasts.
Mesenchymal cells in between osteoid may be
spindle shaped , round , oval or polygonal .
May be uniform or pleomorphic with bizarre
hyperchromatic nuclei and frequent mitotic
figures. Sometimes giant cells are present.
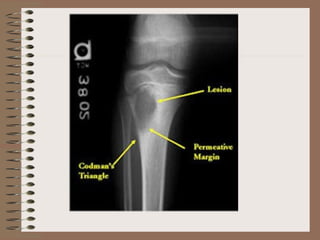
X ray –The tumour elevates the perostium to
form cod man triangle formed by the angle
between the elevated periosteum and the
surface of the involved bone . Sunburst pattern
due to osteogenesis within the tumour may also
occur
Parosteal (Juxta cortical ) osteosarcoma arise
from the external surface of the bone
( parosteal or juxta cortical means outer to
the cortex ) This has better prognosis
Ewing Sarcoma
It isa primary malignant small round cell
tumour of bone . 2nd
commonest tumour in
children. Patients are between 10 & 15 years
of age . The majority of tumours show t ( 11;
22 ) (q 24; q 12) translocation . Femur , tibia
and pelvis are the favoured sites . Arises from
the medullary cavity. Occurs most often in
diaphysis
Gross : Tan white with areas of haemorrhage
and necrosis
38.
Microscopy: Sheets ofinform small
round cells with scant cytoplasm which
appears clear since it is rich in glycogen
(PAS+ ve ). Stroma is minimal . Necrosis
may be prominent
X ray Onionskin appearance due to layers
of reactive bone deposited
Metastatic tumours arethe most common
form of skeletal malignancy . Pathways of
spread include 1) direct extension 2)
lymphatic or hamatogenous dissemination 3)
intraspinal seeding
Majority of skeletal metastases
orginate from cancers of the
prostate ,breast ,kidney & lungs.In children
metastases to bone originate from
Neuroblastoma ,Wilms tumour , osteosarcoma
, Ewing sarcoma & rhabdomyo sarcoma.
Metastatic Disease
41.
Arthritis
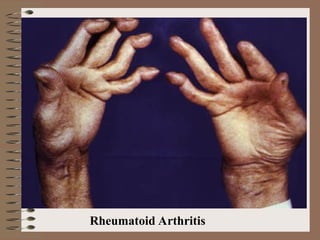
Rheumatoid Arthritis
It isa chronic systemic inflammatory
disorder that may affect many tissue & organs
– skin, blood vessels, heart , lungs & muscles –
but principally attack joints
skeletal metastases are typically multifocal .
Most involve axial skeleton
Diseases of Joints
42.
It produces anonsuppurative proliferative
and inflammatory synovitis that often progress
to destruction of the articular cartilage and
ankylosis of the joints. It is an autoimmune
disorder
Morphology :- Joints :- There is synovial
hypertrophy with lymphocytic infiltration and
Pannus formation finallycausing fibrosis
ankylosis leading to bony ankylosis .
Skin - 25% of patients show
rheumatoid nodules Blood vessels- show
vasculitis
Pathogenesis: RA is an autoimmune disease
triggered by exposure of a genetically
susceptible host to unknown arthritogenic
antigen. CD4 helper cells and other lymphocytes
liberate inflammatory mediators & cytokines
that ultimately destroy the joints
45.
Osteoarthritis
Also called degenerativejoint disease. Is the
most common type of joint disease. It is
characterised by progressive erosion of
articular cartilage. Osteoarthritis is
considered to be an intrinsic disease of
cartilage in which biochemical & metabolic
alterations in individuals with genetic
susceptibility result in its breakdown. It is not
an inflammatory disease.
46.
Primary osteoarthritis (idiopathic)is an aging
process. Secondary osteoarthritis has some
underlying predisposing cause like injuries to a
joint, developmental deformity of a joint,
systemic diseases like diabetes , ochronosis or
haemochromatosis or marked obesity.
Pathogenesis : multifactorial disease with
genetic & environmental components. Net
impact of multiple genes like those involved in
prostaglandin metabolism &WTN signalling.
Environmental factors related to ageing &
biochemical stress obesity muscle strength,
joint stability & alignment. Association with
aging is strong. Increases exponentially
47.
beyond 50. chondrocytesare at the centre of the
process & phases include 1) chondrocyte injury
2) chondrcyte proliferation 3) chondrocyte drop
out with subchondral bone changes.
Morphology : In the early stages chondrocytes
proliferate forming clusters. Water content of
matrix increases, proteoglycans decrease
causing fibrillation& cracking of matrix as
superficial layers of cartilage & collagen
molecules are degraded. Chondrocytes die&
cartilage & subchondral bone are sloughed off
forming loose bodies (joint mouse)
48.
Exposed subchondral boneis smoothened
out due to friction giving polished ivory
appearance ( bone eburnation). Sclerosis of
underlying cancellous bone occur & small
fracture develop. Mushroom shaped
osteophyte develop at articular margin
Clinical course: Deep achy pain that worsens
with use, morning stiffness , crepitus &
limitation of range of movement. Joints
commonly involved include hip, knee, lower
lumbar & cervical vertebrae, proximal &
distal interphalangeal joints etc . Heberdens
nodes common in women are osteophytes at
distal interphalangeal joints
49.
Synovial Sarcoma
It isso named because it was once believed
to recapitulate synovium, but the cell of origin
is still unclear . Less than 10 % are intra
articular . Most occurs in 20s to 40s . Majority
develop in deep soft tissues in vicinity of large
joints especially knee & thigh . Biphasic
synovial sarcoma shows dual line of
differentiation ie epithelial like & spindle cells



































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












