This document discusses bipolar disorders, including prevalence, diagnostic criteria, and treatment. Some key points:
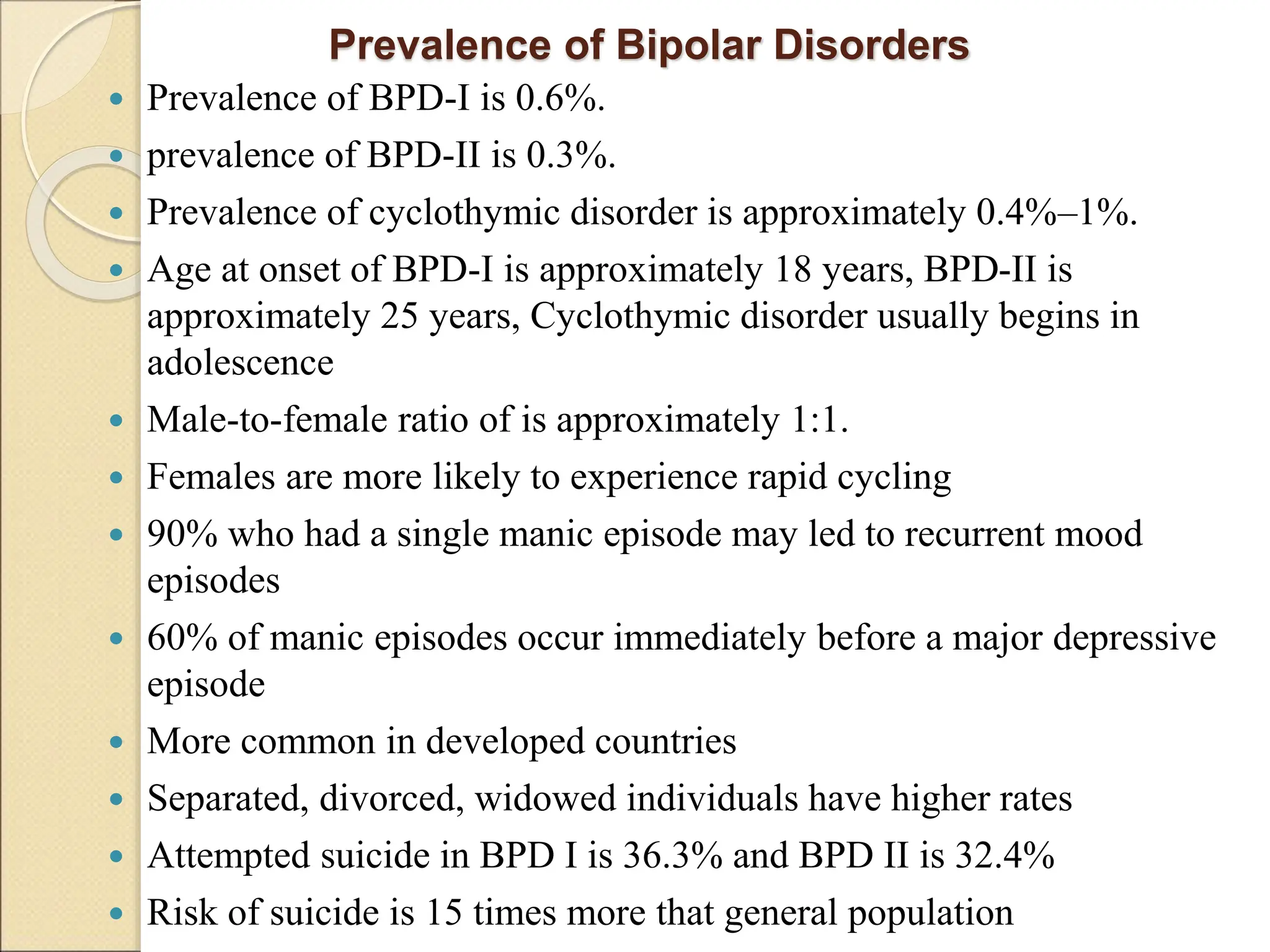
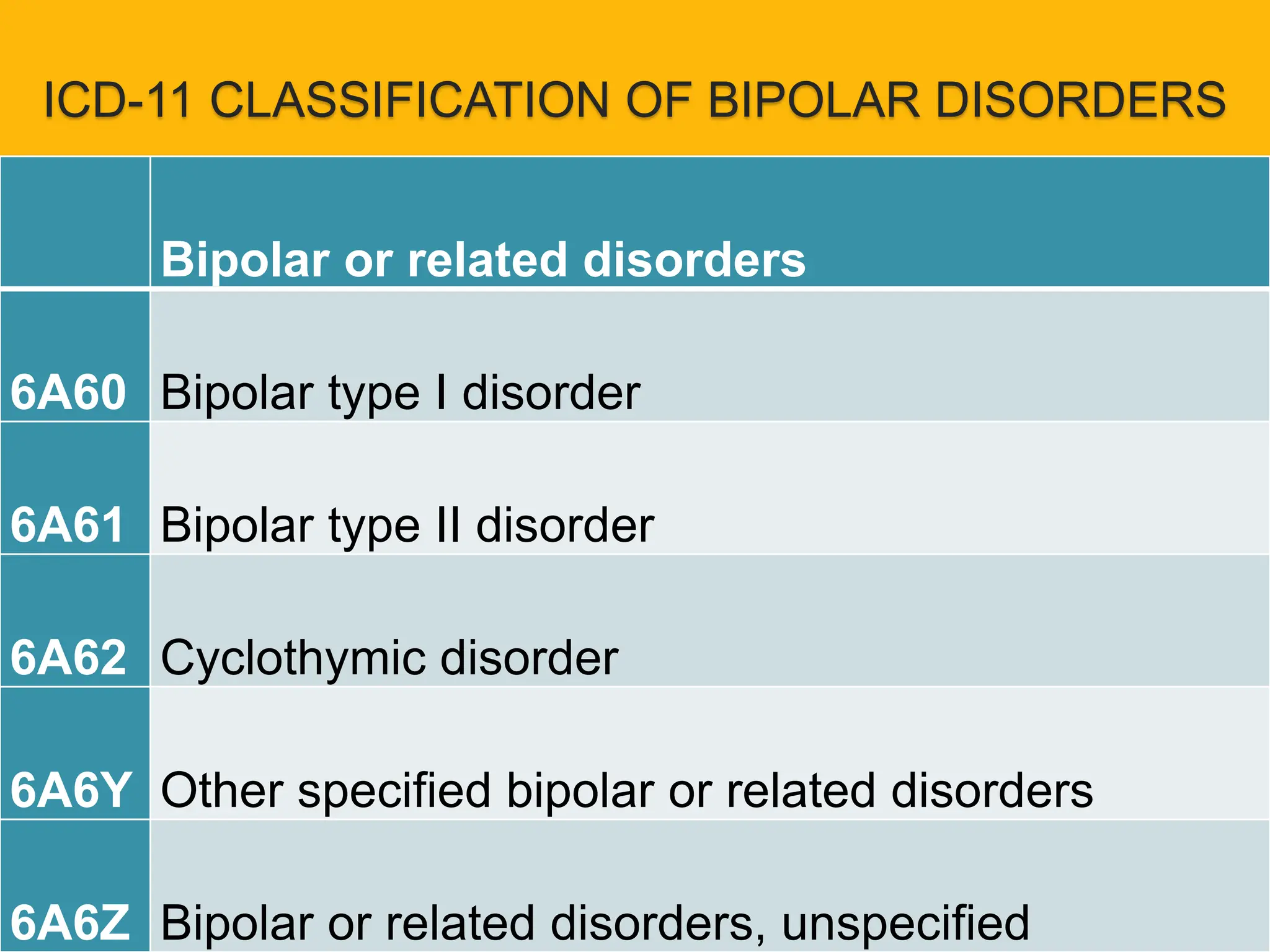
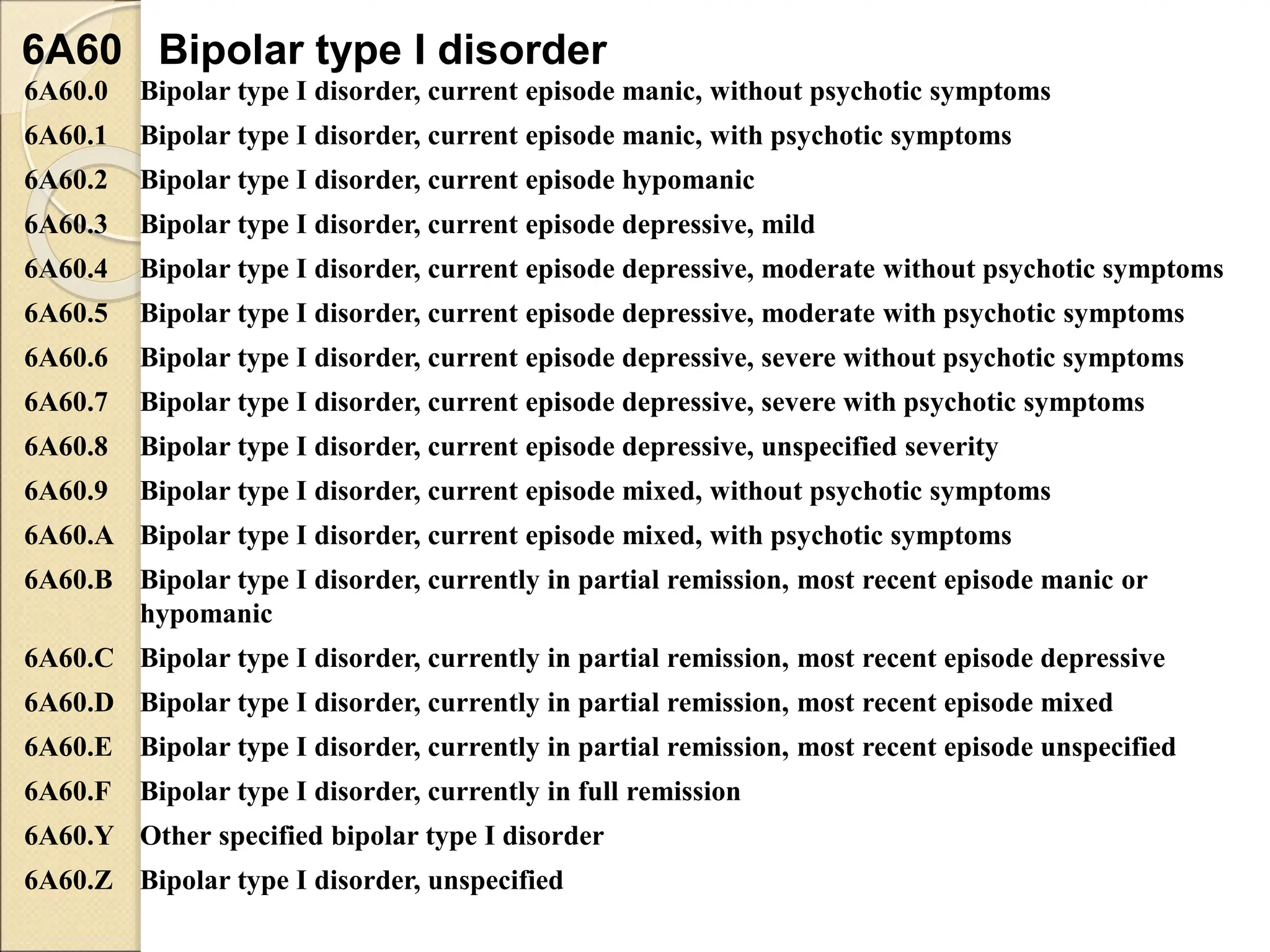
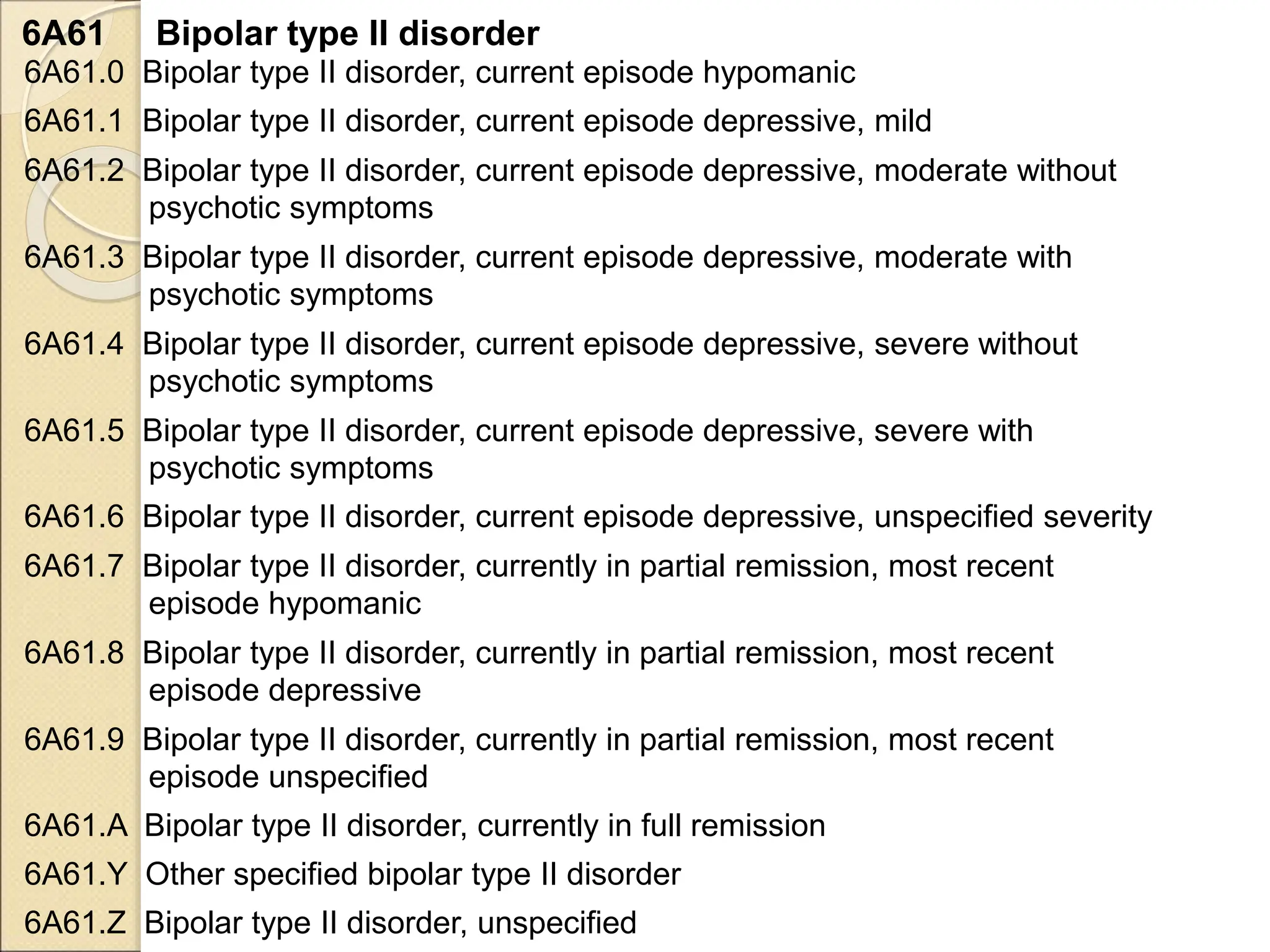
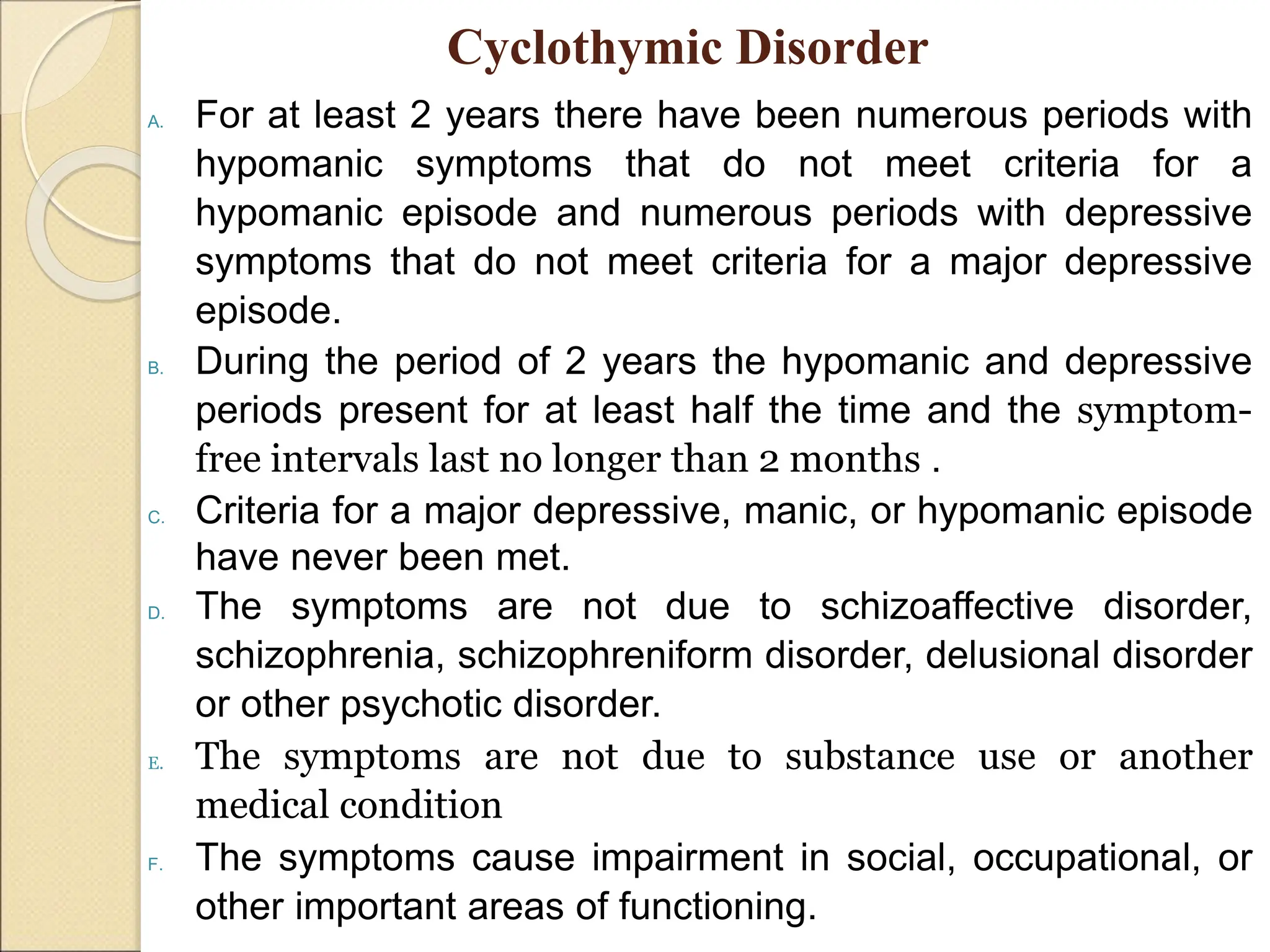
- Bipolar I disorder is characterized by manic or mixed episodes, while Bipolar II involves hypomanic and depressive episodes but no full mania. Cyclothymic disorder involves numerous periods of hypomania and depression over at least two years.
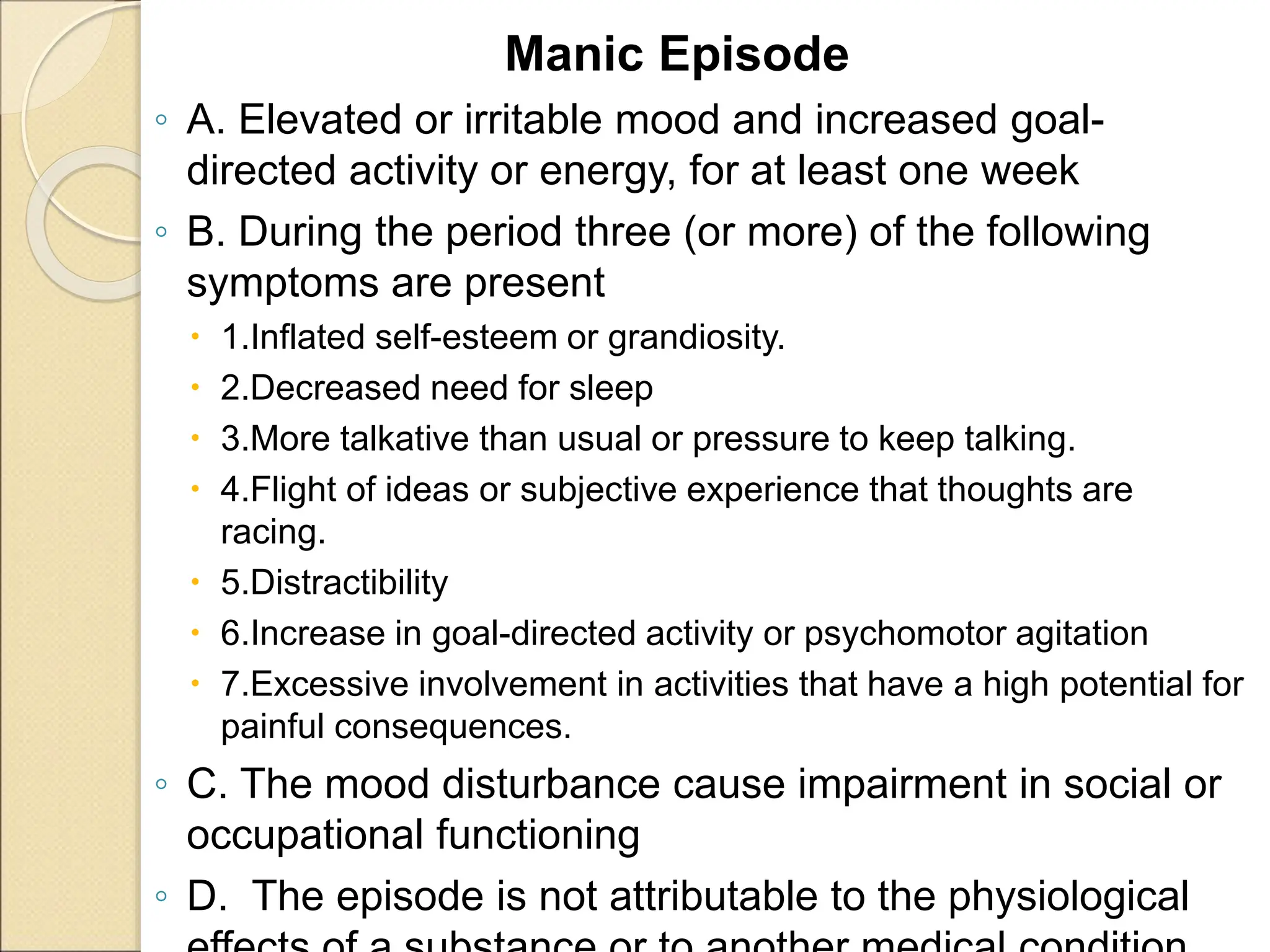
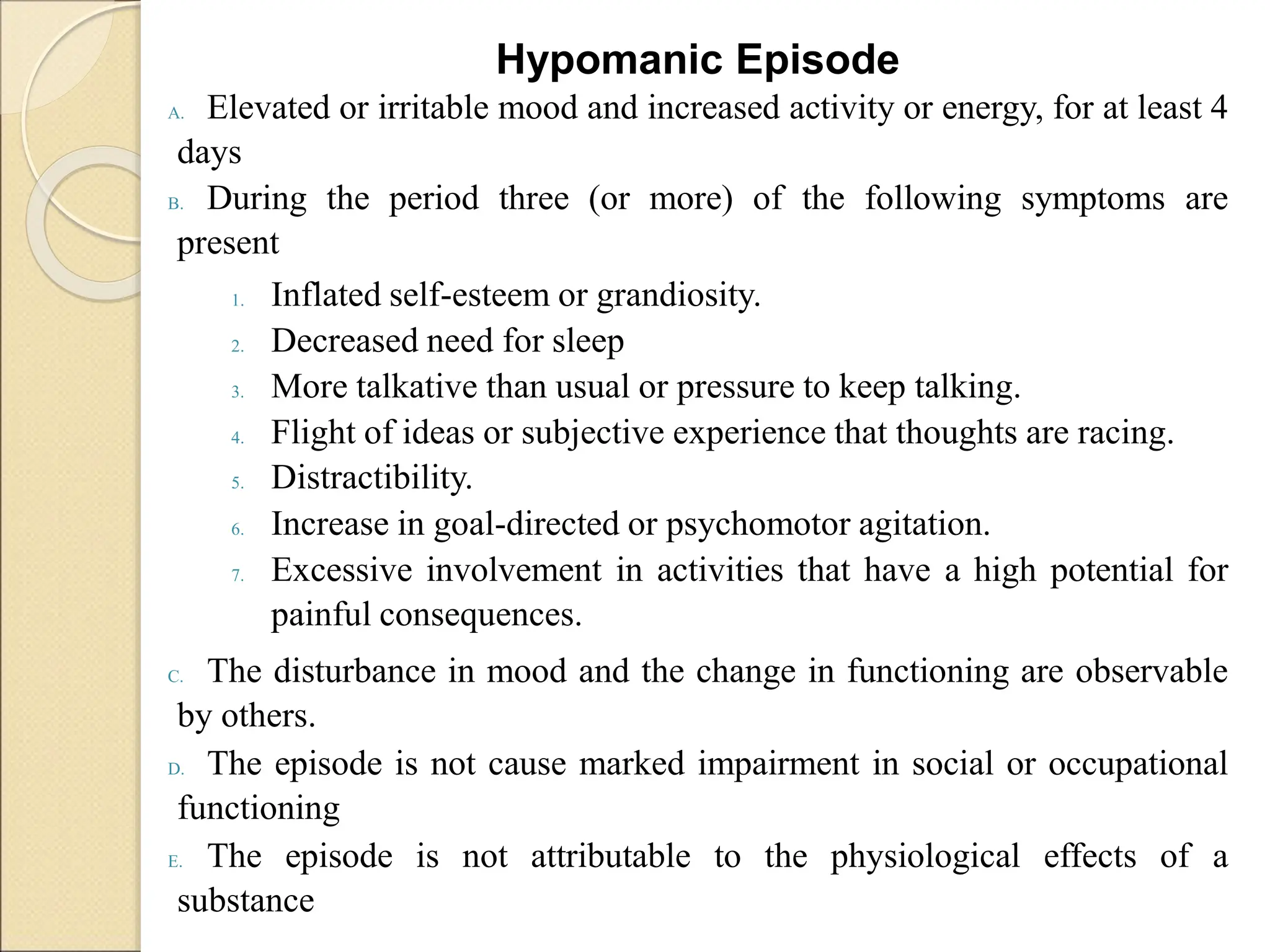
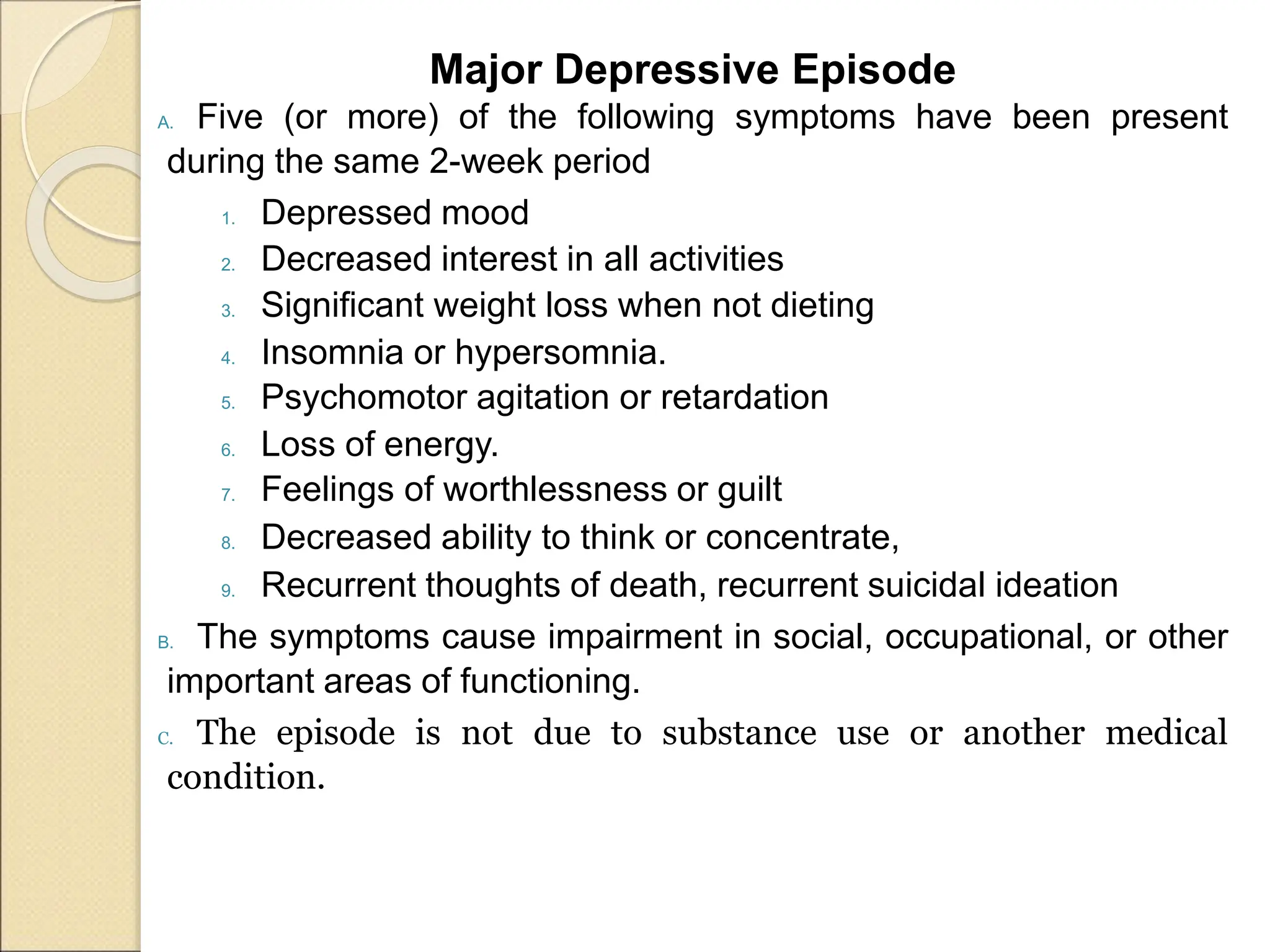
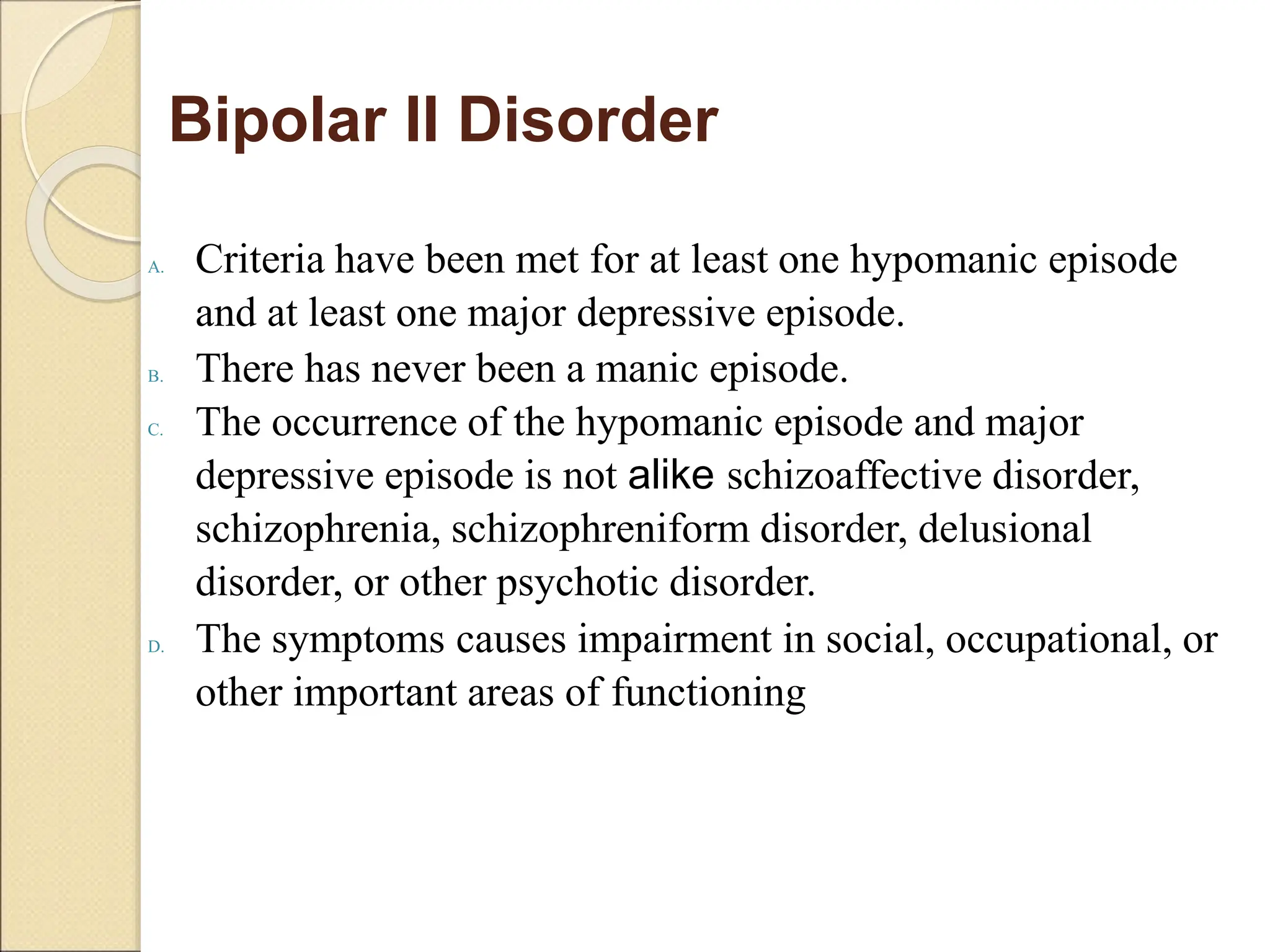
- Diagnostic criteria for manic, hypomanic, and depressive episodes are provided. Genetic and neurobiological factors may contribute to bipolar disorders.
- Treatment depends on the current phase, and may include mood stabilizers, antipsychotics, antidepressants, psychotherapy, and electroconvulsive therapy. Nursing care focuses on safety























![Lesson 3 MOOD DISODRERS [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lesson3mooddisodrersautosaved-250928022615-d2257896-thumbnail.jpg?width=640&height=640&fit=bounds)


































