Definition
● A biomaterialis defined as any
natural or synthetic
substance/combination of
substances (other than drugs)
which may be employed for any
length of time as a whole or part
of a system, to treat, augment, or
replace any tissue, organ or
function of the body, in order to
maintain or improve the quality
of life of the individual.
- American national institute of health
6.
Classification of biomaterial
•Bioinert- minimal interaction with its surrounding tissues,
e.g., stainless steel, titanium
• Bioactive-slight interaction with its surrounding tissues
eg hydroxyapatite, bioglass, glass ceramics
• Bioresorbable-starts to resorb by cellular activity and is
slowly replaced by advancing tissue.
eg. tricalcium phosphate and polylactic polyglycolic acid
7.
Biomaterials used inmedical
and dental applications
1. Metals
2. Ceramics
3. Polymers
4. Natural materials
5. Reinforced materials
9.
Biomimetic material
• Derivedfrom the Greek words bios (life) and
mimesis (imitation)
• Biomimetics refers to the development of
materials and technologies that replicate the
structure and function of natural biological
systems.
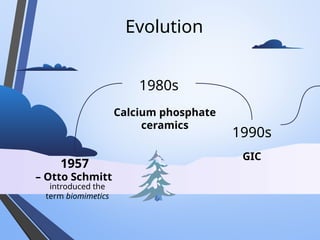
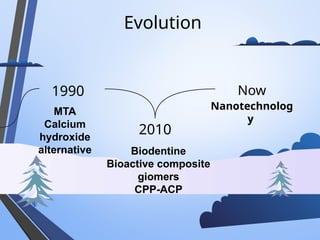
HISTORY OF BIOACTIVE
MATERIALS
Theconcept of bioactive materials originated in the late 1960s when
Hench developed Bioglass®, a silica-based glass capable of forming
a chemical bond with bone.
-Hench LL. The story of Bioglass®. J Mater Sci Mater Med. 2006;17(11):967–
978.
14.
HISTORY OF BIOACTIVE
MATERIALSIN DENTISTRY
• In dentistry, the first bioactive restorative
materials were glass ionomer cements introduced
in the 1970s, primarily valued for their fluoride
release and chemical adhesion.
Journal Club Framework
•Study type: Narrative Review
• Journal: IJJRRD (International journal of
research and reports in dentistry)
• Databases: PubMed, Scopus, Web of Science
• Keywords & inclusion/exclusion criteria defined
• Clinical & translational relevance
20.
Inclusion Criteria
1. Studiesfocused on restorative, preventive, or
regenerative biomimetic materials used in children.
2. Clinical trials, laboratory studies, and systematic
reviews providing evidence for biomimetic
applications dentistry in pediatric
3. Articles addressing material properties such as
bioactivity, remineralization potential, and pulp
response.
21.
Exclusion Criteria
1. Studieslimited to adult populations
without relevance to children.
2. Articles not published in English.
3. Reports with insufficient methodological
detail or lacking peer review.
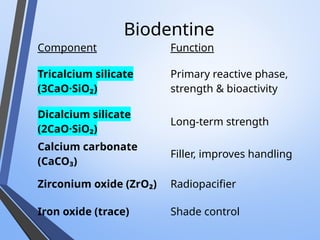
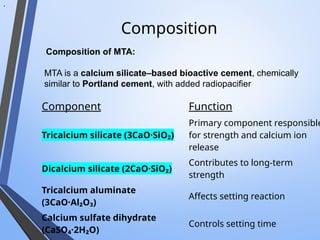
Composition
Component Function
Tricalcium silicate(3CaO·SiO₂)
Primary component responsible
for strength and calcium ion
release
Dicalcium silicate (2CaO·SiO₂)
Contributes to long-term
strength
Tricalcium aluminate
(3CaO·Al₂O₃)
Affects setting reaction
Calcium sulfate dihydrate
(CaSO₄·2H₂O)
Controls setting time
.
. Composition of MTA:
MTA is a calcium silicate–based bioactive cement, chemically
similar to Portland cement, with added radiopacifier
• MTA exhibitsits biological and clinical effects
through hydration, ion release, alkalinity, and
bioactivity.
• a. Hydration Reaction
On mixing with water, MTA undergoes hydration to form:
• Calcium silicate hydrate (C–S–H) gel
• Calcium hydroxide [Ca(OH)₂]
b. Alkaline pH
Initial pH ≈ 10.2, rising to 12.5
Leading to: Antibacterial effect
Neutralizes acidic inflammatory environment
Promotes hard tissue formation
41.
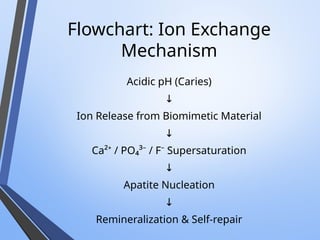
Mechanism of Action
c.Calcium Ion Release
Continuous release of Ca²⁺ ions
Calcium reacts with phosphate ions from tissue fluids →
hydroxyapatite formation
d. Bioactivity & Hard Tissue Induction
Formation of an apatite layer at MTA–dentin
interface
Stimulates: Differentiation of pulp cells into
odontoblast-like cells
Formation of dentin bridge with
minimal tunnel defects
Mechanism of Action(MOA)
A. Hydration Reaction
Tricalcium silicate reacts with water →
Calcium silicate hydrate (C–S–H) gel + Calcium hydroxide (Ca(OH)₂)
C–S–H gel provides
→ mechanical strength
Ca(OH)₂ increases
→ alkalinity (pH 12)
≈
B. Bioactivity & Dentin Bridge Formation
Release of Ca²⁺ ions stimulates:
Differentiation of pulp stem cells into odontoblast-like cells
Formation of reactionary and reparative dentin
Forms a thick, homogenous dentin bridge without tunnel defects (better than
Ca(OH)₂)
C. Apatite Formation
Ca²⁺ reacts with phosphate ions from tissue fluids →
Hydroxyapatite layer formation
Creates a chemical bond with dentin, improving marginal seal
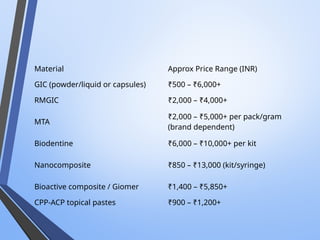
Nanocomposites/Ormocers
Enamel-like optics
• SeptodontEndure Nano Composite – ~₹1,029 (per syringe)
• Other nanocomposite brands available in India:
• 3M Filtek Z350 XT (~₹2,650-₹13,000 depending on kit)
• SDI Luna Nano (~₹850-₹4,650 depending on kit)
• Prime Dent / Fusion (~₹450-₹2,800)
49.
Definition
• Nanocomposites areresin-based restorative
materials in which the filler particles are in the
nanometer range (1–100 nm), either alone or
combined with conventional fillers, to improve
mechanical, esthetic, and biological properties.
50.
Advantage
Nanofillers (5–100 nm)
↓
Highfiller loading
↓
Better stress distribution
↓
↑ Strength + shrinkage
↓
↓
Smooth surface & high esthetics
- Chen M-H. Update on Dental Nanocomposites. J Dent Res. 2010;89:549–560. PubMed
PMID: 20299523.
- Ferracane JL, Stansbury JW, Burke FJ. A review of dental composites: chemistry,
mechanical behavior and clinical performance. Compos Part B Eng. 2021;216:108852.
• Components:
• CaseinPhosphopeptide (CPP)
• Derived from α-casein (contains multiple phosphoseryl
residues – Ser(P)-Ser(P)-Ser(P))
• Acts as a carrier and stabilizer of calcium and phosphate ions
• Amorphous Calcium Phosphate (ACP)
• Non-crystalline, highly soluble form of calcium phosphate
• Provides bioavailable Ca²⁺ and PO₄³⁻ ions
53.
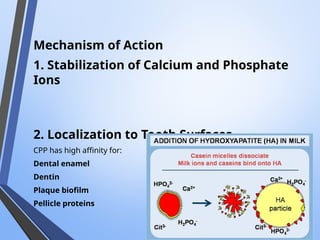
Mechanism of Action
1.Stabilization of Calcium and Phosphate
Ions
2. Localization to Tooth Surfaces
CPP has high affinity for:
Dental enamel
Dentin
Plaque biofilm
Pellicle proteins
54.
Biomimetic Materials inPulp
Therapy
• Indirect & direct pulp
capping
• Pulpotomy in primary teeth
• Regenerative endodontics
in immature teeth
• Shift: protection →
regeneration
Preventive Biomimetic
Strategies
• CPP-ACPfor white spot lesions
• Bioactive pit & fissure sealants
• Sustained fluoride systems
• Nano-hydroxyapatite technologies
Bishayi D, Srinivasan A, Mahabala KY, Natarajan S, Rao A, Nayak AP. A novel application of a bioactive material as a pit
and fissure sealant: in vitro pilot study evaluating the sealing ability and penetration. Eur Arch Paediatr Dent. 2023
Apr;24(2):195-201. doi: 10.1007/s40368-022-00773-z. Epub 2022 Dec 28. PMID: 36575275; PMCID: PMC10192183.
57.
Relevance in Childrenwith
SHCN
• Atraumatic placement
• Reduced chairside time
• Enhanced enamel repair
• Improved treatment
acceptance
Article review
Strengths:
• Comprehensivereview
• Clear biological rationale
Identified Research Gaps:
• Need for pediatric RCTs
• Long-term survival analysis
• Cost-effectiveness studies
• Standardized outcome measures
66.
Conclusion
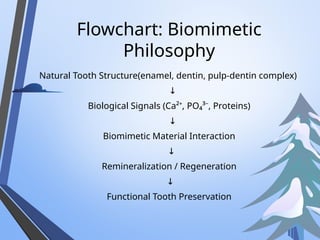
Biomimetic dentistry bridgesbiology and
technology.
In pediatric patients, it enables regeneration-
oriented, minimally invasive, and durable care.
Key References
• AravindaVSS et al. IJRRD. 2025.
• Torabinejad M, et al. Mineral trioxide aggregate: a comprehensive literature review
—Part I. J Endod. 19Banerjee A. Br Dent J.
• Schwendicke F. Adv Dent Res.
• McDonald RE, Avery DR, Dean JA. Dentistry for the Child and Adolescent. 10th ed.
Elsevier; 2016.
• Bishayi D, Srinivasan A, Mahabala KY, Natarajan S, Rao A, Nayak AP. A novel
application of a bioactive material as a pit and fissure sealant: in vitro pilot study
evaluating the sealing ability and penetration. Eur Arch Paediatr Dent. 2023
Apr;24(2):195-201. doi: 10.1007/s40368-022-00773-z. Epub 2022 Dec 28. PMID:
36575275; PMCID: PMC10192183.
• Chen, Ruhua & Xie, Yimeng & Ma, Liang & Li, Bing & Yao, Wei. (2024). Non-
collagenous protein analog-induced biomimetic mineralization strategy to
restore the dentin interface. Biomedical Physics & Engineering Express. 10.
10.1088/2057-1976/ad81fe.
• Hench LL. The story of Bioglass®. J Mater Sci Mater Med. 2006;17(11):967–978.
Editor's Notes
#54 Capping Pulpo- mta biomimetic bridge repair
Regene- mta biodentine- stimu root format
#57 Enamel hypoplasia, caries susceptibility,xerostomia, medical and behavioural limitations















![• MTA exhibits its biological and clinical effects
through hydration, ion release, alkalinity, and
bioactivity.
• a. Hydration Reaction
On mixing with water, MTA undergoes hydration to form:
• Calcium silicate hydrate (C–S–H) gel
• Calcium hydroxide [Ca(OH)₂]
b. Alkaline pH
Initial pH ≈ 10.2, rising to 12.5
Leading to: Antibacterial effect
Neutralizes acidic inflammatory environment
Promotes hard tissue formation](https://image.slidesharecdn.com/jcbiomimeticmaterials-260121142112-abc53292/85/Biomimetic-Materials-in-pediatric-dentistry-40-320.jpg)