This document provides information about diabetes mellitus, including:
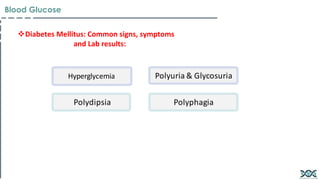
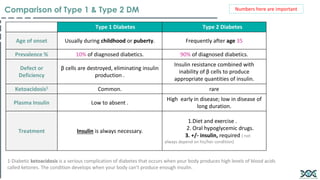
1. It compares Type 1 and Type 2 diabetes, noting differences in age of onset, prevalence, defects/deficiencies, risk of ketoacidosis, plasma insulin levels, and typical treatment approaches.
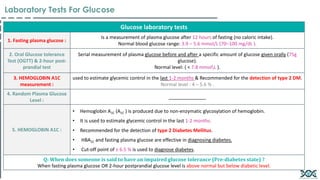
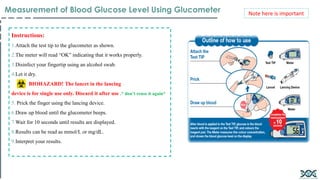
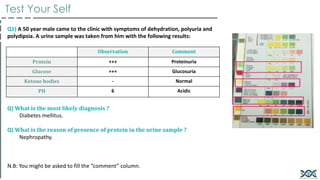
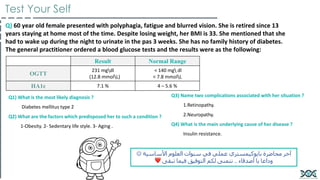
2. It outlines various laboratory tests used to diagnose and monitor diabetes, including fasting plasma glucose, oral glucose tolerance test, hemoglobin A1c, and random plasma glucose tests.
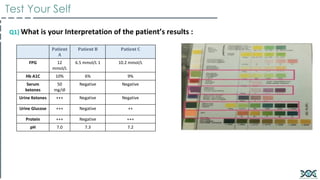
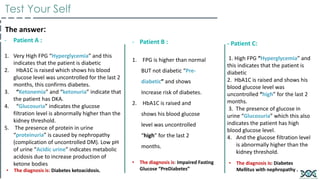
3. It provides criteria for diagnosing diabetes based on results of fasting plasma glucose, oral glucose tolerance, and hemoglobin A1c tests.

![Categories Of Increased Risk of DM & Diagnosis Of DM
Test performed/ - Normal Pre-diabetes Diabetes
Fasting Plasma Glucose
(FPG)
Less than 100 mg/dl
FPG or IFG 1 : 100 - 125
mgdl
5.6 - 6.9 mmol/L
(fasting= No caloric intake for at least
8hs) 126 mgdl and over 7 mmol/L
and over
2 hours post glucose on the
75-g OGTT
Less than 140 mg/dl
OGGT or IGT2
[ 2 : 140 – 199 mgdl 7.8 –
11.0 mmol/L ]
200 mgdl and over 11.1 mmol/L and
over
HA1C Less than 5.7% 5.7% - 6.4 % 6.5% and over
Random Plasma Glucose
Level
_____ _____
200 mg/dl and over 11.1 mmol/L and
over
+ signs and symptoms of
hyperglycemia or hyperglycemic crisis
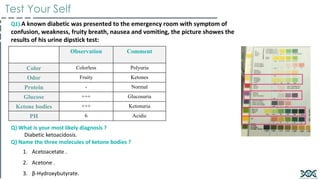
• Ketone Bodies:
• They produce by the liver and utilized for energy production by peripheral tissues . ( common in type I DM)
1. Acetone (exhaled by lungs, gives characteristic smell in diabetic ketoacidosis patients).
2. Acetoacetate.
3. β-Hydroxybutyrate.
4. Produced by the liver and utilized for energy production by peripheral tissues.
1- IFG: impaired fasting
glucose
2- IGT: impaired glucose
tolerance
Criteria For Diagnosis of Diabetes Mellitus](https://image.slidesharecdn.com/biochemistrypracticalbloodglucose-240313164505-3179b2be/85/Biochemistry-practical-Blood-glucose-pdf-6-320.jpg)












































![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)


