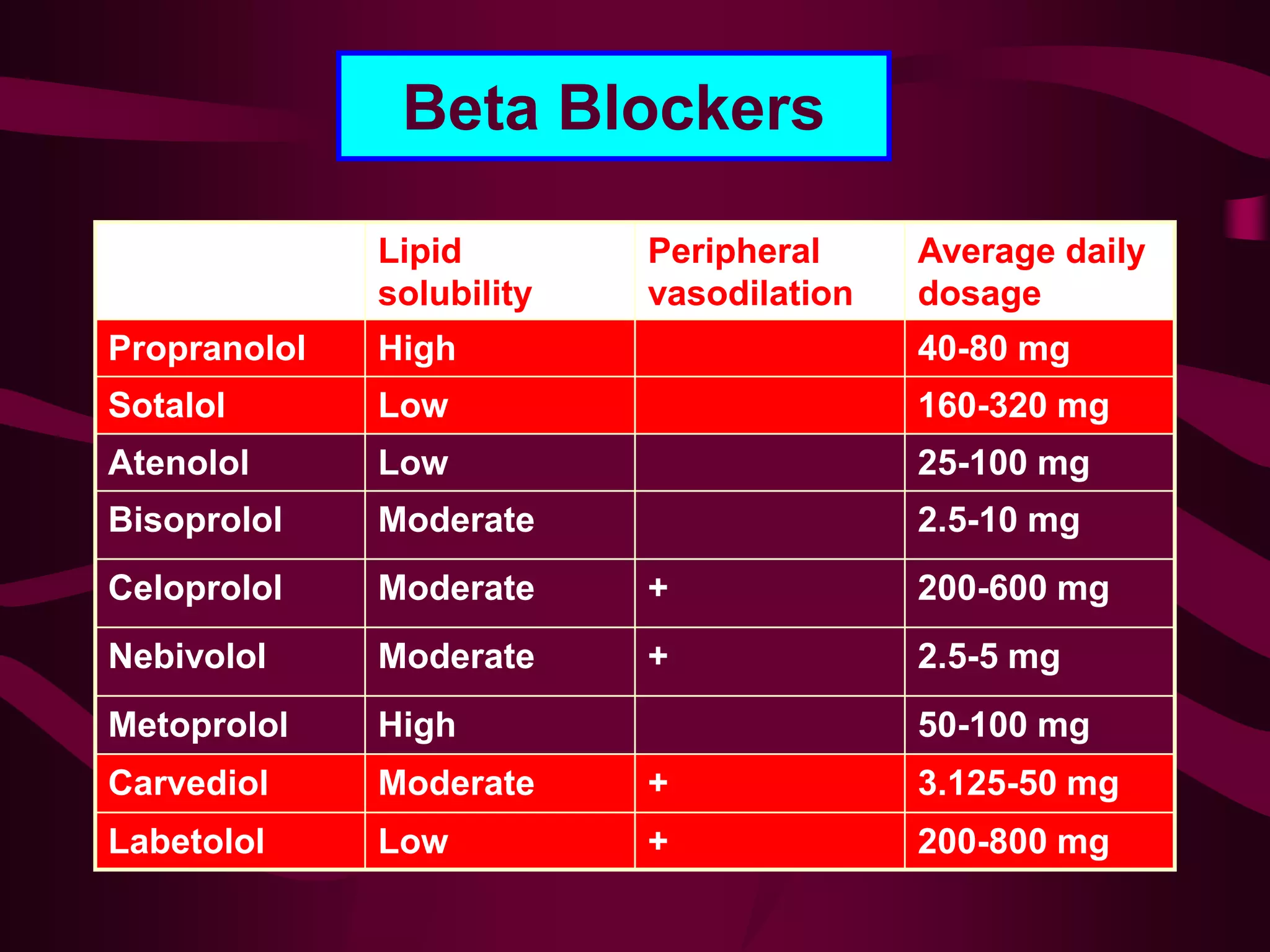
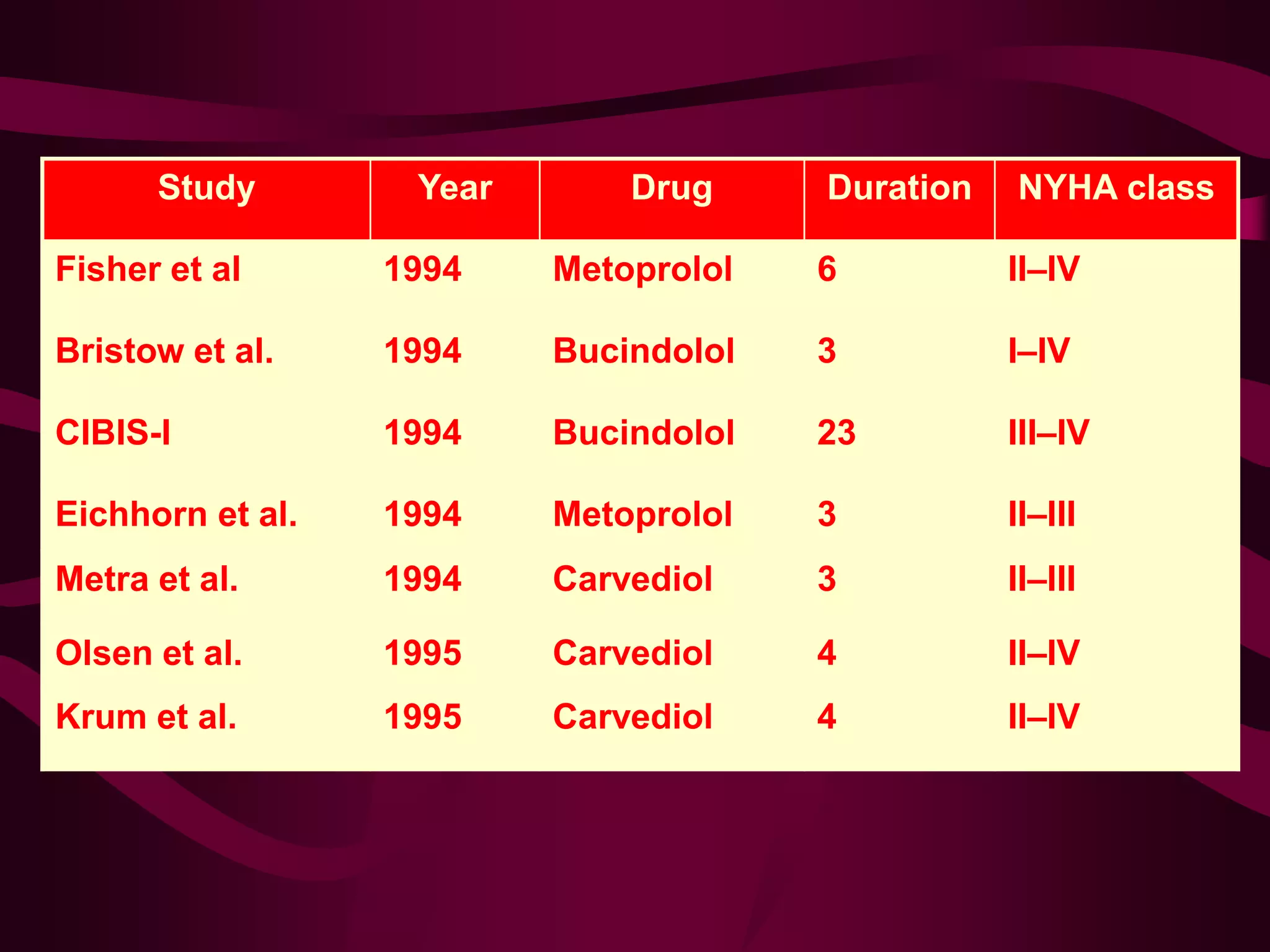
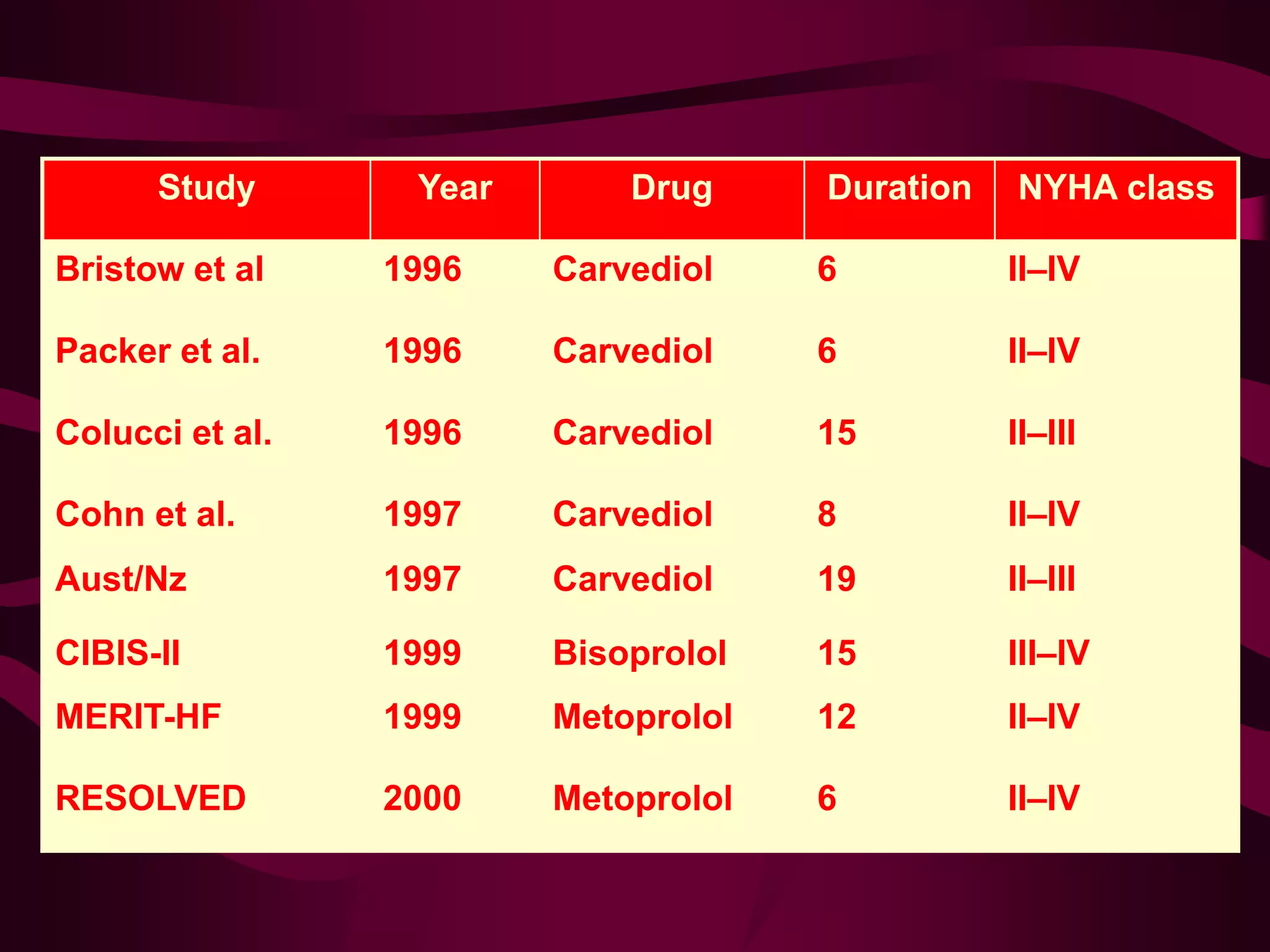
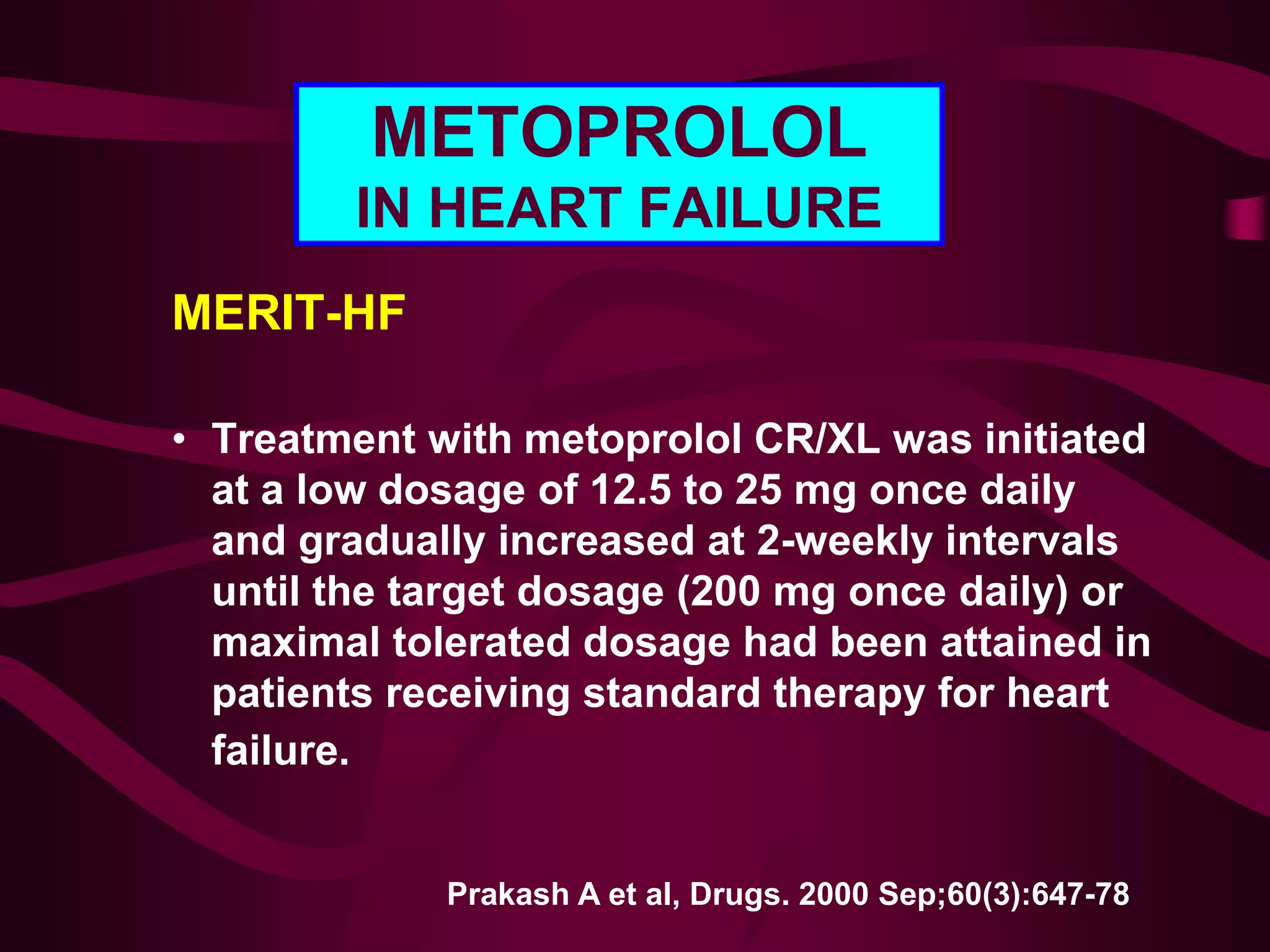
Beta blockers were first introduced in the 1960s and have since been shown to be effective for treating several cardiovascular conditions like hypertension, angina, heart failure, and arrhythmias. Key events included the development of propranolol in 1962 and the differentiation of beta receptors into subtypes. Large clinical trials demonstrated beta blockers reduce mortality in acute myocardial infarction, hypertension, and heart failure. While earlier non-selective beta blockers had more side effects, later trials showed cardioselective beta blockers are well tolerated and do not negatively impact patients with mild to moderate asthma.