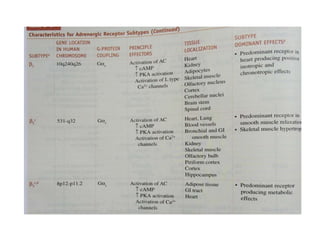
This document discusses β-adrenoceptor modulation in therapeutics. It begins with an introduction to the autonomic nervous system and its regulation of involuntary functions. It then covers the history of discoveries about sympathetic neurotransmitters like norepinephrine and parasympathetic neurotransmitters. The document discusses the classification of α and β adrenergic receptors, their properties, and the ranking of agonists. It also covers receptor regulation mechanisms like desensitization, up/down regulation, and denervation supersensitivity. Finally, it states that drugs affecting the β-adrenergic system are used therapeutically and concludes with references.