Siri Sarva, DMD
Oraland Maxillofacial Surgery, PGY-3
Howard University Hospital
Local Anesthesia Basics
2.
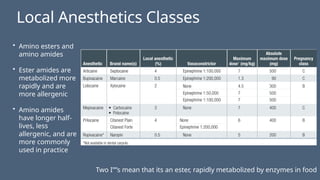
Local Anesthetics Classes
•Amino esters and
amino amides
• Ester amides are
metabolized more
rapidly and are
more allergenic
• Amino amides
have longer half-
lives, less
allergenic, and are
more commonly
used in practice
Two I””s mean that its an ester, rapidly metabolized by enzymes in food
3.
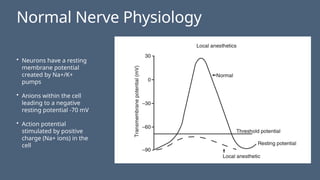
Normal Nerve Physiology
•Neurons have a resting
membrane potential
created by Na+/K+
pumps
• Anions within the cell
leading to a negative
resting potential -70 mV
• Action potential
stimulated by positive
charge (Na+ ions) in the
cell
4.
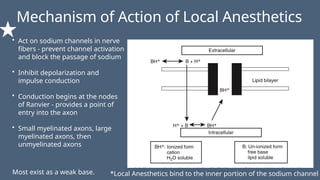
Mechanism of Actionof Local Anesthetics
• Act on sodium channels in nerve
fibers - prevent channel activation
and block the passage of sodium
• Inhibit depolarization and
impulse conduction
• Conduction begins at the nodes
of Ranvier - provides a point of
entry into the axon
• Small myelinated axons, large
myelinated axons, then
unmyelinated axons
*Local Anesthetics bind to the inner portion of the sodium channel
Most exist as a weak base.
5.
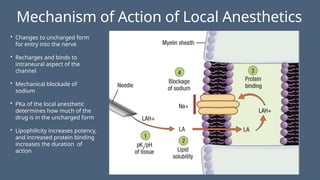
Mechanism of Actionof Local Anesthetics
• Changes to uncharged form
for entry into the nerve
• Recharges and binds to
intraneural aspect of the
channel
• Mechanical blockade of
sodium
• PKa of the local anesthetic
determines how much of the
drug is in the uncharged form
• Lipophilicity increases potency,
and increased protein binding
increases the duration of
action
6.
Components of LocalAnesthetic
• Local Anesthetic
• Vasoconstrictor
• Methylparaben - bacteriostatic preservative in multidose vials. Not so much in cartridges.
• Bisulfites - preservative used in dental cartridges that contain vasoconstrictor (Concern
with patients with Sulfa Drug Allergy.)
• Latex Allergies: The diaphragm contains latex
7.
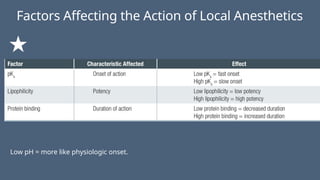
Factors Affecting theAction of Local Anesthetics
Low pH = more like physiologic onset.
8.
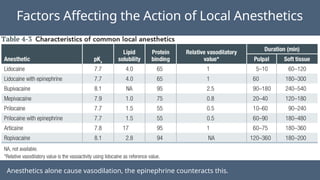
Factors Affecting theAction of Local Anesthetics
Anesthetics alone cause vasodilation, the epinephrine counteracts this.
9.
• Onset: pKadetermines the speed of onset
• Potency: the lipid solubility determines the potency
• Duration: protein binding determines the duration of
• Metabolism: the faster the metabolism, the lower the toxicity
• half Life Lidocaine 90 minutes
• Half life septocaine 20-40 minutes
• Half life bupivacaine 200 minutes
Compare half life and toxicity
10.
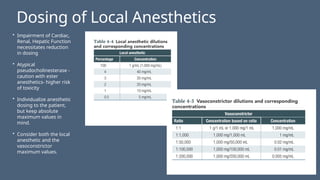
Dosing of LocalAnesthetics
• Impairment of Cardiac,
Renal, Hepatic Function
necessitates reduction
in dosing
• Atypical
pseudocholinesterase -
caution with ester
anesthetics- higher risk
of toxicity
• Individualize anesthetic
dosing to the patient,
but keep absolute
maximum values in
mind.
• Consider both the local
anesthetic and the
vasoconstrictor
maximum values.
11.
Dosing Calculations
• Whatis the maximum amount of 2% Lidocaine with 1:100,000 epinephrine (in milligrams)
that can be administered to a healthy 150 lb man?
• Convert Pounds to kg by dividing the weight in lbs by 2.2 which gives us 68 kg
• The maximum dose of 2% lidocaine with 1:100K Epi. In the adult patient is 7 mg/kg
• Multiply 68 kg x 7 mg/kg
• 477 mg
12.
Dosing Calculations
• Howdo you calculate the amount in milligrams of any anesthetic
and vasoconstrictor in a given solution?
• For local anesthetics, for every 1% of solution, there is 10 mg/mL
of local.
• Total milligrams = % of the solution x 10 x total milliliters
• For every 1:100,000n there is 0.1 mg/mL
• Total milligrams = ratio times total milliliters
• 1.8 mL dental cartridge of 2% Lidocaine with 1:100,000
Epinephrine has 20 mg/mL of lidocaine and 0.01 mg/mL of
epinephrine
• This totals 36 mg of lidocaine and 0.018 mg of epinephrine
13.
Dosing Calculations
• Whatis the maximum number of dental cartridges of 2% Lidocaine with 1:100,000 that
can be given to this 150 lb individual?
• 13 cartridges
• Standard dental cartridge contains 36 mg lidocaine (1.8 mL)
• 477/36 mg/cartridge - 13.25 cartridges
14.
Dosing Calculations
• Howmany dental cartridges of lidocaine or mepicavaine can be administered to a 30 lb
child?
• Maximum pediatric dose weight of child in lb divided by 150 x maximum adult dose in
mg
• 2% Lidcaine with 1:100K Epinephrine = 2.6 cartridges
• 3% Mepivacaine = 1.6 cartridges
15.
Additional Dosing Considerations
•Infant local dosing varies because infants have an increased cardiac output, leading to increased
absorption; immaturity of plasma proteins, causing increased amounts of free local anesthetic in the
plasma; and slower plasma clearance from immature hepatic enzymes
• Hepatic blood flow decreases by 10% per decade, enzymatic function is impaired, and albumin quantity is
decreased.
• Renal clearance is reduced because elderly patients have decreased renal blood flow (10% per decade in
adult years) and decreased glomerular filtration, causing prolongation of metabolite elimination.
• elderly patients who have impaired cardiac function or dysrhythmias, bupivacaine should be used
cautiously because it is more cardiotoxic than comparable doses of lidocaine are.
• Pregnancy and lactation are not contraindications to the administration of local anesthetic. As noted
earlier, the lipophilicity of a local anesthetic allows it to cross the placenta. Lidocaine, prilocaine, and
ropivacaine are the only three local anesthetics that have a class B drug classification by the US Food and
Drug Administration. Lower lipid profiles.
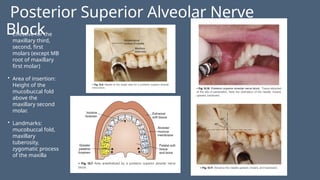
Posterior Superior AlveolarNerve
Block
• Effective for the
maxillary third,
second, first
molars (except MB
root of maxillary
first molar)
• Area of insertion:
Height of the
mucobuccal fold
above the
maxillary second
molar.
• Landmarks:
mucobuccal fold,
maxillary
tuberosity,
zygomatic process
of the maxilla
22.
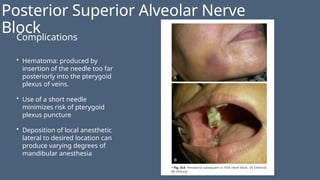
Posterior Superior AlveolarNerve
Block
Complications
• Hematoma: produced by
insertion of the needle too far
posteriorly into the pterygoid
plexus of veins.
• Use of a short needle
minimizes risk of pterygoid
plexus puncture
• Deposition of local anesthetic
lateral to desired location can
produce varying degrees of
mandibular anesthesia
23.
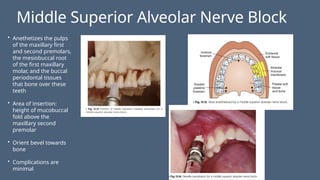
Middle Superior AlveolarNerve Block
• Anethetizes the pulps
of the maxillary first
and second premolars,
the mesiobuccal root
of the first maxillary
molar, and the buccal
periodontal tissues
that bone over these
teeth
• Area of insertion:
height of mucobuccal
fold above the
maxillary second
premolar
• Orient bevel towards
bone
• Complications are
minimal
24.
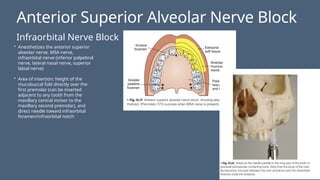
Anterior Superior AlveolarNerve Block
Infraorbital Nerve Block
• Anesthetizes the anterior superior
alveolar nerve, MSA nerve,
infraorbital nerve (inferior palpebral
nerve, lateral nasal nerve, superior
labial nerve)
• Area of insertion: height of the
mucobuccal fold directly over the
first premolar (can be inserted
adjacent to any tooth from the
maxillary central incisor to the
maxillary second premolar), and
direct needle toward infraorbital
foramen/infraorbital notch
25.
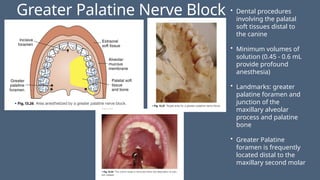
Greater Palatine NerveBlock • Dental procedures
involving the palatal
soft tissues distal to
the canine
• Minimum volumes of
solution (0.45 - 0.6 mL
provide profound
anesthesia)
• Landmarks: greater
palatine foramen and
junction of the
maxillary alveolar
process and palatine
bone
• Greater Palatine
foramen is frequently
located distal to the
maxillary second molar
26.
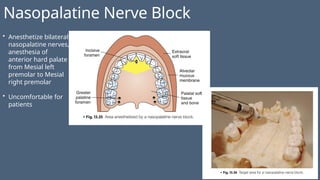
Nasopalatine Nerve Block
•Anesthetize bilateral
nasopalatine nerves,
anesthesia of
anterior hard palate
from Mesial left
premolar to Mesial
right premolar
• Uncomfortable for
patients
27.
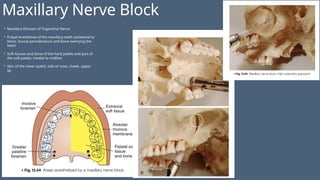
Maxillary Nerve Block
•Maxillary Division of Trigeminal Nerve
• Pulpal Anesthesia of the maxillary teeth ipsilateral to
block, buccal periodontium and bone overlying the
teeth
• Soft tissues and bone of the hard palate and part of
the soft palate, medial to midline
• Skin of the lower eyelid, side of nose, cheek, upper
lip
28.
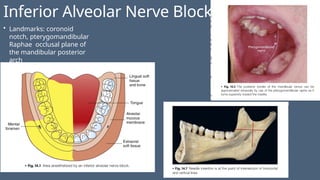
Inferior Alveolar NerveBlock
• Landmarks: coronoid
notch, pterygomandibular
Raphae occlusal plane of
the mandibular posterior
arch
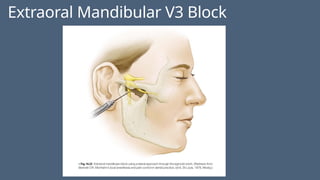
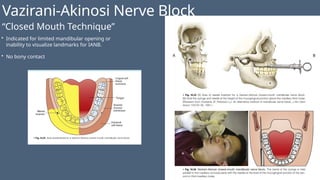
Vazirani-Akinosi Nerve Block
“ClosedMouth Technique”
• Indicated for limited mandibular opening or
inability to visualize landmarks for IANB.
• No bony contact
32.
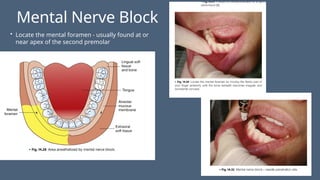
Mental Nerve Block
•Locate the mental foramen - usually found at or
near apex of the second premolar
33.
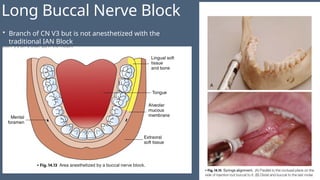
Long Buccal NerveBlock
• Branch of CN V3 but is not anesthetized with the
traditional IAN Block
34.
Local Anesthesia Complications
•Local Anesthesia Toxicity: Normally with bupivicane and ropivicaine - Treated with Intra-lipid, to
administer via IV 1ml/kg. 100ml b
• CNS Symptoms - Light-headedness, tinnitus, perioral numbness, confusion
• Muscle Twitching, auditory and visual hallucinations
• Tonic-clonic seizure, unconsciousness, respiratory arrest
• Cardiac Symptoms- hypertension, tachycardia,
• Decreased contractility and cardiac output, hypotension
• Sinus bradycardia, ventricular dysrhythmias, respiratory arrest
• Methemoglobinemia ( More common to Prilocaine, have to use a lot). Treated 1mg/kg of
methylene blue IV.
35.
Local Anesthesia Complications
Management
•Benzodiazepines - drug of choice for seizure control
• Intralipid - reverses the cardiac and neurological effects of local anesthesia toxicity by
extracting lipid soluble molecules from plasma = 1.5 mL/kg bonus IV. 3 doses
• Phentolamine - also known as oraverse
• Methylene Blue 1 mg/kg
• Vitamin C
#2 The two classes of local anesthetics are amino esters and amino amides. They differ in the type of cross-linkage between the aromatic ring and the tertiary amine that forms the basic chemical structure of all local anesthetics. In general, compared with amides, ester local anesthetics are metabolized more rapidly because of plasma cholines- terase metabolism and are more allergenic. Amides undergo hepatic metabolism, resulting in longer half-lives; are less allergenic; and are the primary anesthetics used in clinical practice.
Amide anesthetics are commonly recognized by the two instances of the letter i in the name. Clinically relevant amides include lidocaine, bupivacaine, mepivacaine, prilocaine, articaine, and ropivacaine (Table 4-1). Esters have one i in the name and include tetracaine, chloroprocaine, procaine, benzocaine, and cocaine. Benzocaine and cocaine are primarily used for topical application. Other common topical formulations helpful for intravenous cath- eter or laceration site anesthesia in children are EMLA (eutectic mixture of the local anesthetics lidocaine 2.5% and prilocaine 2.5%) and LET (lidocaine 4%, epinephrine 0.1%, and tetracaine 0.5%).
#4 Local anesthetics affect sodium ion channels in nerve fibers by preventing channel activation and mechanically blocking the passage of sodium. These actions inhibit depolarization and impulse conduction. Conduction begins at the nodes of Ranvier, the gaps in the myelin sheath that encircles the nerve axons. These gaps give the anes- thetic a point of entry into the axon (Fig 4-1). In the uncharged, basic form, local anesthetics can cross through the lipid-rich axon and gain access to the ion channel binding sites from the axoplasmic aspect of the nerve termi- nal. Inside the nerve terminal, the anesthetic changes to the charged form through ionization, and the cationic form of the anesthetic attaches to the receptor site. Binding is improved when the channel is in the activated or inactivat- ed form and is decreased when channels are in the resting state, a characteristic known as frequency-dependent blockade.2 The small myelinated axons (Aγ and Aδ) are anesthetized first, the larger myelinated axons (Aα and Aβ) are anesthetized next, and unmyelinated axons (C fibers) are anesthetized last.
#5 Local anesthesia mechanism of action. The local anesthetic agent (LA) is introduced in charged form (LAH+) outside the nerve (1), changes to uncharged form for entry into the nerve (2), and recharges and binds to the intraneural as- pect of the channel (3), resulting in a mechanical blockade of sodium passage (4). Note that in step 1, the pKa of the LA will determine how much of the drug is in the uncharged form. As the pKa nears the physiologic pH of 7.4, a greater portion of the drug is in the uncharged form, which enters the lipid bilayer. Thus, pKa affects the onset of action. In step 2, lipophilicity dictates potency. Highly li- pophilic LA will readily cross the lipid bilayer. In step 3, protein binding determines the duration of action. As protein binding increases, the LA will have a longer duration of action due to prolonged binding to the sodium channel.
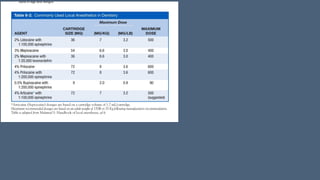
#7 action of local anesthetics is influenced by pKa, lipid solubility, protein binding, and vasoactivity (Tables 4-2 and 4-3). The pKa of a solution, which is the pH at which 50% of the drug is in its charged form and 50% is in its uncharged form, dictates the onset of action of a drug. A local anesthetic exists in two forms: charged, or ionized, and uncharged, or nonionized. Each has opposing chemical features. The charged form is hydrophilic and tends to bind the protein channel, whereas the uncharged form is lipophilic and tends not to bind the protein channel but can more readily cross the lipid bilayer than the charged form can. Assuming that the pH of tissue is 7.4, a local anesthetic with a pKa of 7.4 would have 50% of the drug in the charged, ionized form and 50% in the uncharged, nonionized form in tissue. The pKa of most local anesthetics is > 7.4; therefore, > 50% of the drug is in the charged form. A higher pKa means that a greater proportion of the drug is in the charged form, which does not enter the axon readily. Conversely, a lower pKa means that a greater proportion of the drug is in the uncharged form, which is able to enter the axoplasmic space and bind the ion channel. Thus, the onset of action is more rapid with a lower pKa. For example, lidocaine, which has a pKa of 7.9, has a faster rate of onset than bupivacaine, which has a pKa of 8.1. Infection causes tissue acidity (lower pH), which increases ionization, thus resulting in the presence of more of the charged form of an anesthetic and slower uptake into nerves. High volumes of an anesthetic of comparatively lower concentration in a confined tissue space can accelerate onset of anesthesia because of increased pressure for mass diffusion through adjacent tissue.3